Opioid Analgesics Nursing Considerations: A Comprehensive Clinical Guide (2026)
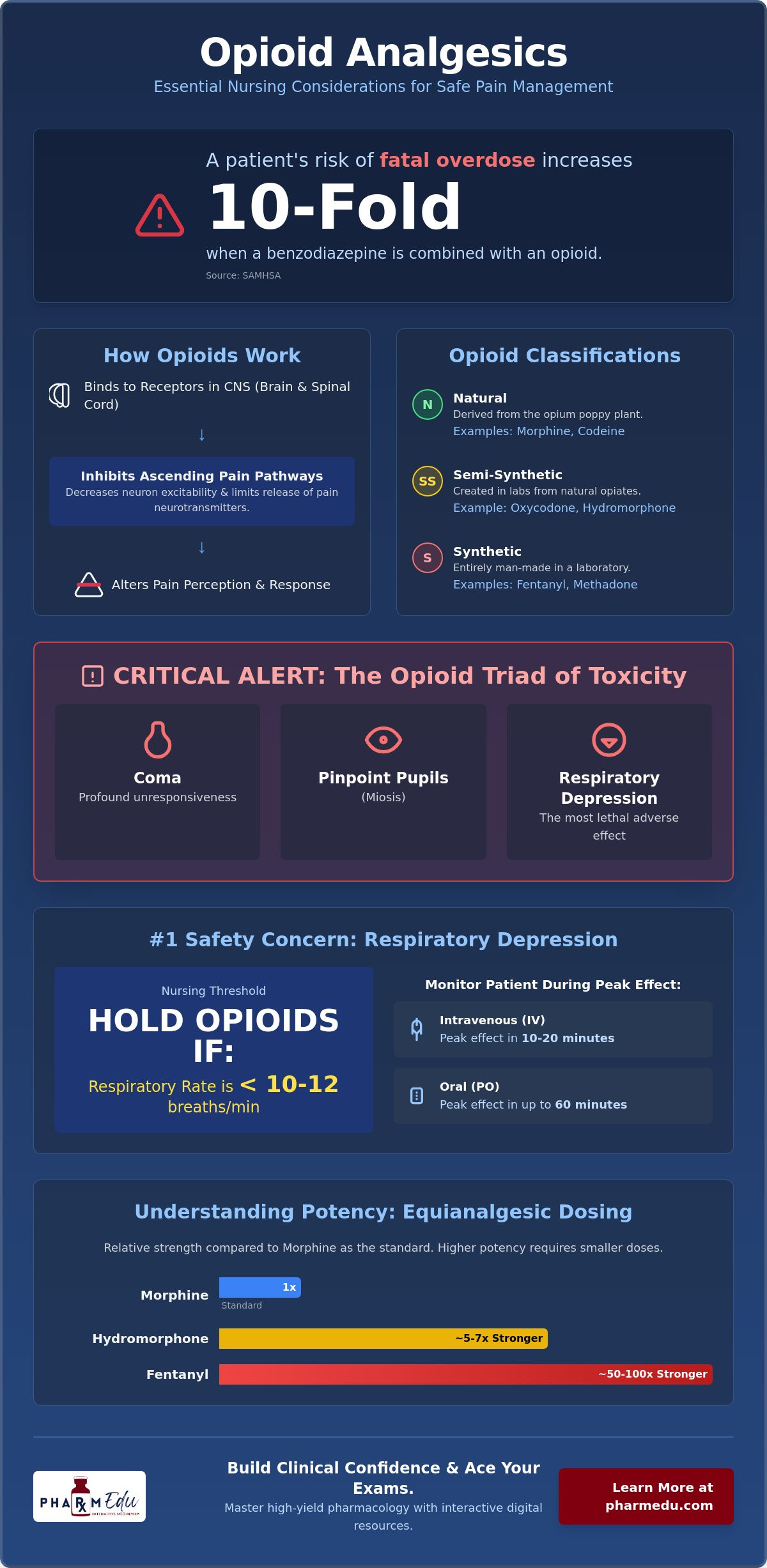
Did you know that a patient’s risk of fatal overdose increases tenfold when a benzodiazepine is combined with an opioid prescription? This startling statistic from recent SAMHSA data highlights why clinical vigilance is your most powerful tool at the bedside. It’s completely natural to feel overwhelmed by the shifting landscape of pain management, especially with the 2026 FDA Education Blueprint introducing stricter standards for patient monitoring and updated terminology for substance use disorders.
We understand that mastering opioid analgesics nursing considerations isn’t just about passing a pharmacology quiz; it’s about the safety of those under your care. This comprehensive guide promises to transform your anxiety into clinical confidence by bridging the gap between complex pharmacology and real-world application. You’ll gain a clear mastery of Mu-receptor mechanisms, safety protocols, and the high-yield facts required for board exam success. We will break down the essential nursing process, from the initial assessment to the latest multimodal analgesia trends, ensuring you’re fully prepared for the challenges of modern practice.
Key Takeaways
- Understand how Mu-receptor agonists alter pain perception and learn to distinguish between natural, semi-synthetic, and synthetic opioids for precise clinical application.
- Identify the critical “opioid triad” of symptoms and prioritize interventions for respiratory depression, which remains the most lethal adverse effect in opioid therapy.
- Master the complexities of equianalgesic dosing and compare the relative potencies of high-risk medications like Fentanyl and Hydromorphone against Morphine standards.
- Apply the systematic nursing process to every stage of care, ensuring that opioid analgesics nursing considerations such as pre-administration assessments and the “Six Rights” are strictly maintained.
- Build the pharmacology foundation necessary for both clinical excellence and board exam success by utilizing structured, high-yield digital learning resources.
Understanding Opioid Analgesics: Mechanisms and Classifications
Opioid analgesics represent a powerful class of medications designed to manage moderate to severe pain by interacting with specific receptors in the central nervous system. These agents don’t just “block” pain; they fundamentally alter how the brain perceives and responds to painful stimuli. Understanding these Opioid Mechanisms and Classifications is a vital step for any clinician. Nurses must distinguish between natural opiates, such as morphine and codeine, and semi-synthetic options like oxycodone. Fully synthetic opioids, including fentanyl and methadone, are entirely man-made and often carry much higher potencies. These distinctions are critical because they dictate specific opioid analgesics nursing considerations regarding metabolism, onset of action, and duration of effect.
The primary mechanism of action involves the inhibition of ascending pain pathways. When an opioid binds to its target receptors in the spinal cord and brain, it decreases the excitability of neurons and limits the release of neurotransmitters like substance P. We categorize these drugs by their relative strength to guide safe administration. Weak opioids, such as codeine or tramadol, are typically utilized for moderate pain. In contrast, strong opioids like fentanyl and hydromorphone are reserved for severe acute pain or end of life care where high potency is required for comfort.
The Mu-Receptor and Pain Modulation
Opioids interact with three primary receptor types: Mu, Kappa, and Delta. The Mu-receptor is the most significant for clinicians because it provides the most profound analgesia. However, its activation is also responsible for the most dangerous side effects, such as respiratory depression, euphoria, and physical dependence. Kappa receptors contribute to spinal analgesia and sedation, while Delta receptors are involved in modulating emotional responses to pain. A ceiling effect refers to a pharmacological phenomenon where increasing a drug’s dose past a certain point provides no additional pain relief but significantly increases the risk of toxicity.
Agonists, Antagonists, and Mixed Agents
Full agonists, like morphine, bind heavily to Mu-receptors and produce a maximal biological response. They lack a ceiling effect, which allows the dosage to be titrated upward indefinitely until the patient’s pain is controlled or side effects become unmanageable. On the opposite end of the spectrum, antagonists like naloxone have a high affinity for Mu-receptors but produce no response. They’re used to “bump” agonists off the receptor sites during an overdose. Mixed agonist-antagonists provide a more complex challenge. These agents can trigger immediate, severe withdrawal symptoms if they’re administered to a patient who is already opioid-dependent. Mastering these pharmacological nuances is a core component of opioid analgesics nursing considerations in both emergency and postoperative settings.
Critical Adverse Reactions and Nursing Alerts
Managing the potent effects of these medications requires a high level of clinical suspicion. The “opioid triad” represents the most critical presentation of toxicity: coma, pinpoint pupils (miosis), and profound respiratory depression. Recognizing this trio immediately is a cornerstone of opioid analgesics nursing considerations, especially in high-acuity environments. Beyond acute toxicity, nurses must stay vigilant for the 10-times greater risk of fatal overdose that occurs when opioids are combined with benzodiazepines, as highlighted in recent FDA Black Box warnings and 2026 clinical updates.
Respiratory Depression: The Primary Safety Concern
Respiratory depression is the most lethal adverse effect and serves as the primary limiting factor in dosage titration. Clinical protocols typically establish a nursing threshold for holding opioids at a respiratory rate of less than 10 to 12 breaths per minute. Monitoring timing is essential; you must assess the patient during the drug’s peak effect. For intravenous administration, this peak often occurs within 10 to 20 minutes, whereas oral routes may take up to 60 minutes to reach maximum impact. If you suspect depression, your immediate steps include stimulating the patient, holding further doses, and preparing for the administration of naloxone. For a deeper dive into these protocols, the Clinical Guidelines for Opioid Analgesics provide exhaustive monitoring frameworks.
Gastrointestinal and Genitourinary Effects
While patients often develop tolerance to nausea and sedation within a few days, they never develop a tolerance to opioid-induced constipation (OIC). This makes proactive bowel management a non-negotiable part of opioid analgesics nursing considerations. Nurses should initiate a “mush and push” regimen involving stool softeners and stimulants immediately upon the start of therapy. Urinary retention is another common but frequently overlooked complication. Assessing for bladder distension or utilizing a bladder scanner can prevent the need for more invasive catheterization. If nausea persists, consider slow IV administration or pre-treatment with antiemetics to improve patient comfort. Mastering these details is easier with tools like interactive pharmacology flashcards, which help cement these high-yield facts for clinical practice.
In the geriatric population, these side effects are amplified. Older adults are significantly more sensitive to the central nervous system effects of opioids, leading to increased sedation and a high risk for falls. Nurses must “start low and go slow” with this demographic to ensure safety while still providing adequate pain relief. Always evaluate the patient’s environment for safety hazards and ensure they have adequate assistance when ambulating after a dose.
Clinical Applications: Equianalgesic Dosing and Drug Interactions
Equianalgesic dosing is the clinical practice of achieving the same level of pain relief when switching between different medications or routes of administration. It’s a cornerstone of safe practice. Because different opioids possess varying affinities for Mu-receptors, a milligram-to-milligram comparison is never appropriate. For example, 10mg of intravenous Morphine is roughly equivalent to 1.5mg of intravenous Hydromorphone. If a nurse incorrectly assumes a 1:1 ratio, the results could be fatal. These Evidence-Based Nursing Practice for Opioids guidelines emphasize that potency charts are only starting points for individual titration.
Managing Potency and Conversions
When switching a patient from one opioid to another, clinicians must account for incomplete cross-tolerance. This phenomenon suggests that a patient who has developed a tolerance to one opioid may not be equally tolerant to a different one. Therefore, the starting dose of the new medication should typically be reduced by 25% to 50% to prevent unintentional overdose. This is a vital part of opioid analgesics nursing considerations during transitions of care. Never assume that doses are interchangeable across different routes, such as moving from IV to oral administration, as bioavailability varies significantly between agents.
Dangerous Combinations: Benzos and Alcohol
The FDA maintains a strict Black Box Warning regarding the concurrent use of opioids and benzodiazepines. This combination creates a synergistic effect that profoundly depresses the central nervous system, leading to a tenfold increase in overdose risk. Alcohol acts in a similar fashion, severely impairing the drive to breathe. Nurses should also be wary of Meperidine when used with MAOIs, as this can trigger life-threatening serotonin syndrome. Metabolism also plays a role. Many opioids are processed via the CYP450 enzyme system. If a patient is taking a CYP450 inhibitor, such as certain antifungals or antidepressants, the opioid can accumulate to toxic levels. Conversely, if the medication is a pro-drug like codeine, a lack of enzyme activity will result in zero pain relief. These metabolic nuances are why consistent monitoring remains one of the most important opioid analgesics nursing considerations in clinical settings.
Implementing the Nursing Process for Opioid Administration
Applying the nursing process to opioid therapy ensures that pharmacological knowledge translates into safe patient outcomes. It’s the framework that helps you catch potential errors before they reach the patient. When managing opioid analgesics nursing considerations, your assessment must begin before the medication even leaves the dispensing cabinet. This systematic approach is what separates a technician from a clinical professional.
Assessment and Nursing Diagnoses
Vital signs, specifically respiratory rate and blood pressure, provide the baseline for all future interventions. You also need a thorough history of substance use to anticipate potential tolerance or withdrawal issues. The PQRST mnemonic (Provocation, Quality, Region, Severity, Timing) remains the gold standard for characterizing pain. By identifying the specific nature of the pain, you can better advocate for the appropriate analgesic agent. Priority nursing diagnoses for these patients include “Acute Pain” related to the underlying condition and “Risk for Impaired Gas Exchange” related to the drug’s effect on the respiratory center. For students looking to master these concepts for exams, The Ultimate Pharmacology Study Guide for Nursing Students in 2026 offers a deep dive into the clinical reasoning required at the bedside.
Safe Administration and Evaluation
Implementation requires strict adherence to the “Six Rights” of medication administration. When giving IV push opioids, speed is your enemy. For instance, pushing fentanyl too quickly can cause chest wall rigidity, a rare but life-threatening condition where the chest muscles become too stiff for effective ventilation. If your facility utilizes Patient-Controlled Analgesia (PCA), patient education is paramount. The patient, and only the patient, should press the button. This “call don’t fall” approach prevents family members from accidentally overdosing a sleeping patient and ensures the patient remains the primary driver of their own pain management. To see these principles in action, you can explore our clinical case studies which simulate high-pressure administration scenarios.
Evaluation is the final, critical step in the nursing process. You must re-assess the patient’s pain level and respiratory status within 30 to 60 minutes of administration, depending on the route. A successful intervention isn’t just defined by a lower pain score. It’s a patient who is comfortable, alert, and breathing at an appropriate rate without experiencing significant adverse effects. Consistent documentation of these findings is essential for maintaining a safe and effective plan of care.
Mastering High-Yield Pharmacology with PharmEDU
Mastering the vast array of opioid analgesics nursing considerations requires more than just reading a textbook once; it demands a structured, repetitive approach to learning that fits into a busy clinical schedule. PharmEDU serves as a premier digital partner for healthcare students and professionals who need to distill complex pharmacology into actionable knowledge. By providing a centralized platform for clinical excellence, we help you transition from memorizing facts to understanding the physiological “why” behind every intervention. This depth of understanding is what ensures patient safety in high-pressure environments.
Visual learners benefit significantly from our library of over 100 high-yield video vignettes. These short, focused lessons break down drug mechanisms and safety protocols into digestible segments. Instead of wading through hundreds of pages of academic jargon, you can watch a five-minute vignette that clarifies the exact receptors involved in opioid therapy. This visual reinforcement is complemented by interactive pharmacology flashcards and practice quizzes that provide immediate feedback. These tools ensure that your knowledge of dosages, peak effects, and adverse reactions remains sharp long after your initial study session ends.
Micro-Learning for Busy Healthcare Students
Modern clinical rotations don’t leave much room for traditional study sessions. PharmEDU’s mobile-compliant design allows you to review critical facts during clinical breaks or while commuting. This micro-learning approach ensures that you’re always making progress toward your goals without feeling overwhelmed by the volume of material. For those seeking a deeper foundational understanding of drug science, we recommend exploring our Pharmacology: The Comprehensive Guide to the Science of Drugs. We also offer institutional platform licenses for nursing programs, enabling educators to track student progress and integrate high-quality digital content directly into their curriculum for better cohort outcomes.
The PharmEDU Advantage for Board Exams
Success on the NAPLEX or nursing board exams isn’t about knowing everything; it’s about knowing what matters most. Our curriculum is designed by experienced healthcare educators who follow a “high-yield” philosophy. We focus specifically on the information most likely to appear on certification exams, from complex drug-drug interactions to the most critical opioid analgesics nursing considerations. This targeted approach saves you time and reduces the anxiety associated with standardized testing. By aligning our content with current regulatory standards and scientific findings, we ensure you’re prepared for both the exam room and the patient’s bedside. You can Excel in your pharmacology coursework with a PharmEDU Monthly Subscription and gain the clinical confidence needed for a successful career in healthcare.
Elevating Clinical Practice and Patient Safety
Safe administration of Mu-receptor agonists requires more than just a basic understanding of dosage. It demands a vigilant integration of pharmacological knowledge with the systematic nursing process. By mastering opioid analgesics nursing considerations, you transition from simply following orders to becoming a critical safeguard against lethal errors like respiratory depression and the “opioid triad.” You’ve learned how to navigate complex equianalgesic conversions and identify dangerous drug interactions that could compromise patient outcomes. These skills are the foundation of professional excellence and clinical confidence in modern healthcare settings.
Continuous learning is the only way to stay ahead in a rapidly evolving landscape. Our mobile-compliant micro-learning platform is designed specifically by healthcare educators to help you achieve board exam success and bedside mastery. With access to over 100 high-yield video vignettes, you can reinforce your expertise whenever your busy schedule allows. Master pharmacology today with a PharmEDU Subscription and take the next step in your professional journey. We’re here to support your growth and simplify your path to certification. Your commitment to excellence makes all the difference in patient care.
Frequently Asked Questions
What is the most serious adverse effect of opioid analgesics?
Respiratory depression is the most serious and potentially fatal adverse effect of these medications. It occurs because opioids decrease the sensitivity of the brainstem to carbon dioxide levels, leading to a reduced drive to breathe. Vigilant monitoring of respiratory rate and depth is a fundamental component of opioid analgesics nursing considerations, especially during the first 24 hours of therapy or after any significant dose escalation.
How often should a nurse assess a patient after administering an IV opioid?
Nurses should assess patients within 15 to 30 minutes following intravenous administration to capture the drug’s peak effect. While the onset of action for IV opioids is nearly immediate, the maximum respiratory and sedative impact typically occurs within this window. Continuous pulse oximetry or capnography may be required for high-risk patients, such as those with obstructive sleep apnea or those receiving concurrent CNS depressants.
What is the “opioid triad” and why is it a medical emergency?
The “opioid triad” consists of a coma or profound sedation, respiratory depression, and miosis, which refers to pinpoint pupils. This presentation is a medical emergency because it indicates severe toxicity that will lead to hypoxia and cardiac arrest if left untreated. Rapid recognition allows the clinical team to initiate life-saving measures, such as bag-valve-mask ventilation and the immediate administration of opioid antagonists like naloxone.
Can a nurse administer Naloxone without a specific order in an emergency?
In most clinical settings, nurses can administer naloxone under established emergency standing orders or rescue protocols without waiting for a patient-specific physician order. These protocols are designed to prevent delays in care during life-threatening respiratory failure. However, you must always verify your specific facility’s policy and state board of nursing regulations to ensure compliance with local legal frameworks and institutional safety standards.
What is the difference between opioid physical dependence and addiction?
Physical dependence is a predictable physiological adaptation where the body requires the drug to function normally, whereas addiction involves compulsive drug-seeking behavior despite harmful consequences. Patients with chronic pain often develop physical dependence and experience withdrawal if the medication is stopped abruptly. True addiction, now clinically termed Opioid Use Disorder (OUD), involves a loss of control and is a complex psychological condition.
How does equianalgesic dosing help in preventing medication errors?
Equianalgesic dosing provides a standardized framework to compare the potency of different opioids, which prevents dangerous under-dosing or over-dosing during transitions of care. By using a conversion chart, a nurse can ensure that a patient switching from an oral to an intravenous route receives a dose that provides similar pain relief. This precision is essential for maintaining safety and is a key part of opioid analgesics nursing considerations.
What should a nurse do if a patient’s respiratory rate drops below 10 breaths per minute?
If a patient’s respiratory rate falls below 10 breaths per minute, you should immediately attempt to arouse the patient with physical and verbal stimuli. Hold any further doses of the medication and notify the healthcare provider or rapid response team. It’s vital to have naloxone and airway management equipment at the bedside while you continue to monitor the patient’s oxygen saturation and level of consciousness closely.
Why is Fentanyl measured in micrograms while Morphine is measured in milligrams?
Fentanyl is measured in micrograms because it’s approximately 100 times more potent than morphine, meaning a tiny amount produces a massive clinical effect. Measuring such a powerful synthetic opioid in milligrams would lead to significant dosing errors and fatal outcomes. This extreme potency is why fentanyl requires extra layers of verification and slower administration techniques compared to less potent natural opiates like morphine or codeine.