NSAIDs Mechanism of Action and Side Effects: A High-Yield Pharmacology Guide
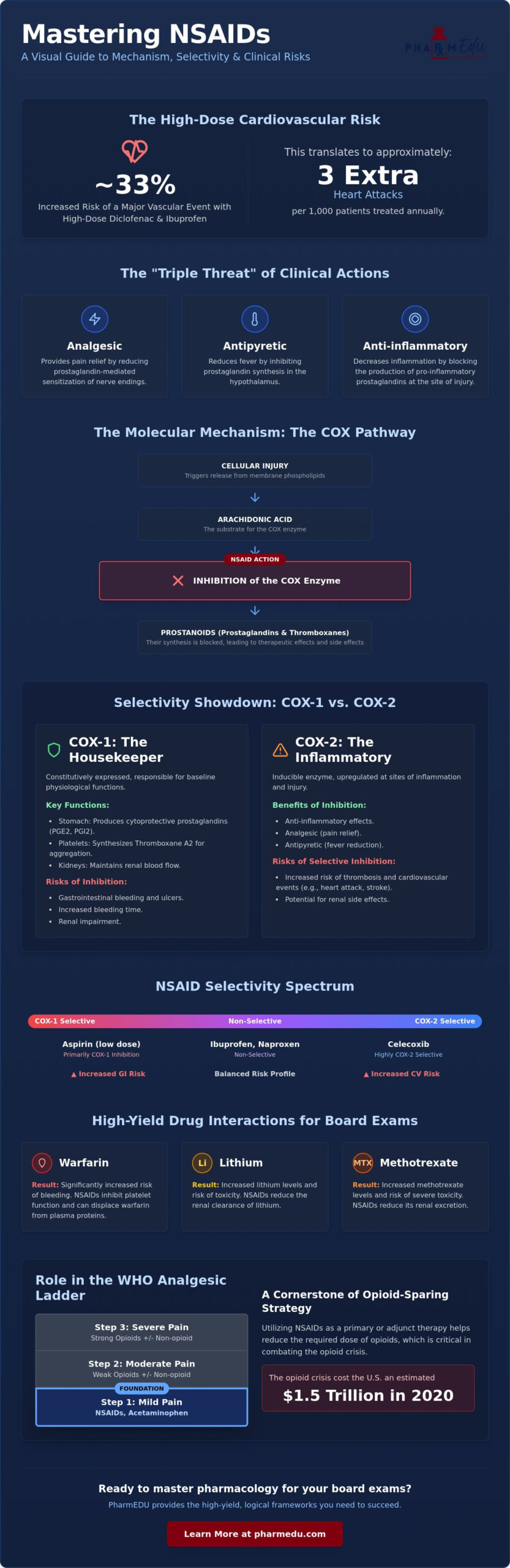
High doses of diclofenac and ibuprofen increase the risk of a major vascular event by about one-third, which translates to approximately three extra heart attacks per 1,000 patients treated annually. While these medications remain a cornerstone of pain management, truly mastering the NSAIDs mechanism of action and side effects requires moving beyond simple rote memorization. You’ve likely felt the frustration of trying to keep COX-1 and COX-2 functions straight while staring at a long list of adverse reactions that often seem to overlap without a clear pattern.
We understand that for a busy professional, clarity is just as vital as accuracy. This high-yield guide promises to provide a logical framework where every clinical risk, from gastrointestinal bleeding to the FDA’s 2024 warning on fixed drug eruptions, becomes a predictable consequence of molecular inhibition. You’ll gain the ability to differentiate between various drug classes and apply this knowledge to complex clinical cases with precision.
Our analysis begins with the molecular pathways of the arachidonic acid cascade before moving into a detailed breakdown of specific clinical risks and recent regulatory shifts. We’ll also examine how these traditional therapies compare to emerging non-opioid alternatives like suzetrigine, ensuring your knowledge is both exam-ready and clinically current.
Key Takeaways
- Identify the “triple threat” of clinical actions: analgesic, antipyretic, and anti-inflammatory, to better categorize the therapeutic utility of various medication classes.
- Map the arachidonic acid cascade to understand how the NSAIDs mechanism of action and side effects are fundamentally rooted in the rate-limiting inhibition of cyclooxygenase enzymes.
- Evaluate the selectivity spectrum between non-selective agents and COX-2 inhibitors to balance inflammatory relief against the risk of gastrointestinal or cardiovascular toxicity.
- Predict specific adverse outcomes, including gastric ulceration, by linking the loss of cytoprotective prostaglandins PGE2 and PGI2 to the molecular inhibition of COX-1.
- Master high-yield pharmacology facts and critical drug-drug interactions involving warfarin, lithium, and methotrexate to ensure readiness for board exams like NAPLEX, NCLEX, and USMLE.
Understanding NSAIDs: Classification and Clinical Utility
A Nonsteroidal anti-inflammatory drug (NSAID) represents a chemically diverse but functionally unified group of compounds used to manage pain and inflammation. While many patients view them as simple over-the-counter remedies, clinicians recognize them as powerful tools that address the “triple threat” of clinical symptoms: pain, fever, and inflammation. This broad utility allows them to treat everything from acute dental pain, as recommended by the American Dental Association’s 2024 guidelines, to chronic conditions like rheumatoid arthritis and osteoarthritis. By targeting the underlying inflammatory response, these drugs provide relief that goes beyond mere symptom masking.
To help dental practices adhere to such clinical guidelines, PractCom provides specialized patient communication tools, including a library of digital informed consent forms and post-treatment instructions that ensure patients are well-informed about their recovery.
It’s essential to differentiate these agents from other common analgesics like acetaminophen. While both are effective for reducing mild pain and lowering fever, acetaminophen lacks the peripheral anti-inflammatory properties that define this class. This distinction is critical when studying the NSAIDs mechanism of action and side effects, as the peripheral inhibition of prostaglandins drives both the therapeutic benefits and the characteristic risks of the drug class. Unlike acetaminophen, which is primarily metabolized in the liver with minimal peripheral COX inhibition, NSAIDs directly impact the site of tissue injury and inflammation.
Therapeutic indications for this class are expansive and include:
- Acute Pain Management: Post-operative pain, dental procedures, and musculoskeletal injuries.
- Chronic Inflammatory Conditions: Long-term management of rheumatoid arthritis, ankylosing spondylitis, and osteoarthritis.
- Fever Reduction: Effective antipyretic action in both adult and pediatric populations.
- Specialized Applications: Treatment of dysmenorrhea and acute gouty flare-ups.
Properly managing these inflammatory conditions is essential for maintaining the physical readiness required for active travel; for instance, those visiting Phuket can explore Try Dive programs as a rewarding way to experience the underwater world safely.
Given the potential for adverse reactions with chronic NSAID use, many individuals consider dietary supplements like Palmitoylethanolamide (PEA) as a complementary approach to managing inflammation; click here to learn more.
Chemical vs. Functional Classification
Clinicians often categorize these drugs by their chemical structure, which influences their pharmacokinetics and niche applications. Salicylates, led by aspirin, are unique for their irreversible inhibition of enzymes. Propionic acid derivatives like ibuprofen and naproxen are perhaps the most common; naproxen is frequently chosen for its longer half-life. Other classes like acetic acid derivatives (indomethacin) and enolic acid derivatives (meloxicam) provide specific clinical advantages, such as potency in gout or a slight preference for COX-2 enzymes. Understanding these chemical nuances is vital for predicting the NSAIDs mechanism of action and side effects in diverse patient populations.
The Role of NSAIDs in the WHO Analgesic Ladder
These medications serve as the foundation of the WHO Analgesic Ladder, occupying Step 1 for managing mild-to-moderate pain. Their role is vital in the context of the opioid crisis, which cost the U.S. $1.5 trillion in 2020. By utilizing these agents in a multimodal analgesia strategy, providers can achieve significant opioid-sparing effects. This approach reduces the required dose of stronger narcotics while maintaining effective pain control for both acute and chronic conditions. Whether used as a primary treatment or an adjunct, they remain a cornerstone of modern pharmacological intervention; for those interested in how tailored nutritional support can further enhance long-term wellness, check out Zenutri Personalised Vitamins.
The Molecular Mechanism of Action: The COX Pathway
Cellular injury triggers the release of arachidonic acid from membrane phospholipids, a process mediated by the enzyme phospholipase A2. This free fatty acid serves as the essential substrate for the cyclooxygenase (COX) enzyme, which acts as the rate-limiting step in the synthesis of prostanoids, including prostaglandins and thromboxanes. The primary mechanism of NSAIDs involves the competitive or irreversible inhibition of the COX enzyme active site, preventing the conversion of arachidonic acid into unstable intermediates. Understanding this disruption is the foundation for mastering the NSAIDs mechanism of action and side effects, as it explains why these drugs are so effective yet carry distinct risks.
Prostaglandin E2 (PGE2) plays a central role in peripheral sensitization by lowering the activation threshold of nociceptors at the site of injury. When tissue damage occurs, PGE2 doesn’t just cause pain; it makes the area hypersensitive to even minor mechanical or chemical stimuli. By inhibiting COX, these drugs reduce PGE2 concentrations, effectively “turning down the volume” of pain signals sent to the central nervous system. Visualizing these complex cascades is often the hardest part of pharmacology, but using interactive pharmacology flashcards can help you solidify these molecular connections for exam day.
COX-1 vs. COX-2: Constitutive vs. Inducible
COX-1 is often described as a “housekeeping” enzyme because it’s expressed constitutively in most tissues, including the stomach and kidneys. It maintains the gastric mucosal barrier and supports healthy renal blood flow. In contrast, COX-2 is an inducible enzyme. Its expression surges in response to inflammatory cytokines, growth factors, and endotoxins. While inhibiting COX-2 provides the desired anti-inflammatory relief, the simultaneous inhibition of COX-1 is the primary driver of NSAID adverse effects, such as gastric erosions and impaired platelet function.
The Aspirin Exception: Irreversible Inhibition
Aspirin stands apart from other agents through its unique biochemical interaction. It covalently modifies the COX enzyme by acetylating a specific serine residue within the active site. This inhibition is irreversible. Because platelets are anuclear and cannot synthesize new proteins, the effect lasts for the entire lifespan of the platelet, which is typically 7 to 10 days. This permanent blockade is why low-dose aspirin is a potent antiplatelet therapy. Higher doses are generally required to achieve generalized anti-inflammatory effects in tissues that can regenerate the enzyme. Mastering these dose-dependent nuances is a frequent requirement for clinical boards and advanced pharmacology certifications.
Selectivity and Comparison: Non-Selective vs. COX-2 Selective
The quest to refine the NSAIDs mechanism of action and side effects led to the development of agents that discriminate between COX isoforms. Traditional NSAIDs were designed to block the production of inflammatory prostaglandins, but their lack of specificity meant they also inhibited the protective enzymes in the gut. This realization triggered an evolutionary shift in drug design, moving from non-selective agents toward COX-2 selective inhibitors. The goal was simple: provide the same level of pain relief while minimizing the risk of life-threatening gastrointestinal toxicity.
It’s a common misconception that “selective” implies “exclusive” action. In reality, selectivity exists on a spectrum defined by relative potencies. At standard therapeutic doses, a selective agent primarily targets one isoform, but as the dose increases, this specificity often diminishes. Clinicians must weigh these pharmacological ratios against the patient’s specific health history. As detailed in NSAIDs: A Comprehensive Review, selecting the right agent involves a delicate balance between protecting the gastric mucosa and safeguarding the cardiovascular system.
Non-Selective NSAIDs (Traditional NSAIDs)
Ibuprofen and naproxen remain the gold standards for general pain management due to their balanced efficacy and safety profiles. However, even these common drugs carry significant risks at high doses. For instance, high doses of ibuprofen are associated with an increased risk of major vascular events by about one-third, which can lead to approximately three extra heart attacks per 1,000 patients annually. Ketorolac stands out as a high-potency analgesic often used for post-operative pain, but its high COX-1 affinity limits its use to a maximum of five days to prevent severe renal or gastric damage. Indomethacin is another specialized non-selective agent, frequently chosen for its effectiveness in treating acute gouty arthritis and closing a patent ductus arteriosus (PDA) in neonates.
COX-2 Selective Inhibitors (Coxibs)
Celecoxib is the primary survivor of the “coxib” class, featuring a unique sulfonamide moiety that requires caution in patients with sulfa allergies. These drugs were specifically engineered for patients with a high risk of peptic ulcers or gastrointestinal bleeding. Despite their GI-sparing benefits, the history of this class is marked by the “Vioxx Lesson.” When rofecoxib (Vioxx) was removed from the market, it highlighted a dangerous cardiovascular trend. By inhibiting COX-2 mediated prostacyclin (a vasodilator and anti-aggregator) without affecting COX-1 mediated thromboxane (a vasoconstrictor and aggregator), these selective agents can tip the physiological balance toward a pro-thrombotic state. This mechanism explains why COX-2 inhibitors are often avoided in patients with established ischemic heart disease.
Adverse Effects: Mechanistic Links to Clinical Risks
The clinical utility of these drugs is often limited by the “Prostaglandin Paradox.” While prostaglandins are the primary mediators of pain and fever, they also serve as essential signaling molecules for maintaining physiological homeostasis in the gut, kidneys, and vascular endothelium. Truly understanding the NSAIDs mechanism of action and side effects means recognizing that most adverse reactions aren’t random toxicities but are direct consequences of inhibiting these protective pathways. When we block the “bad” prostaglandins associated with inflammation, we inevitably interfere with the “good” ones that keep organ systems functioning correctly; in these cases, exploring high-performance health supplements from Herbalgrit.com can be a proactive way to support long-term wellness and vitality.
Gastrointestinal distress remains the most frequent complication encountered in clinical practice. Specifically, NSAIDs cause gastric ulcers by inhibiting COX-1 mediated synthesis of cytoprotective PGE2 and PGI2, which are responsible for stimulating mucus and bicarbonate secretion, maintaining mucosal blood flow, and suppressing gastric acid production. Without these defenses, the stomach lining becomes vulnerable to the corrosive effects of digestive acids. Cardiovascular risks are equally tied to this molecular balance. By suppressing prostacyclin (PGI2) in the endothelium while allowing thromboxane A2 (TXA2) to dominate, some agents create a pro-thrombotic environment that increases the risk of myocardial infarction and stroke. To ensure these risks are managed under professional supervision, patients can visit Unic Advanced Health Services for expert primary care and telehealth consultations.
The “Triple Whammy” of Renal Failure
Renal health depends heavily on prostaglandins to maintain blood flow through the afferent arteriole, especially when systemic perfusion is low. A “triple whammy” occurs when a patient takes an NSAID, an ACE inhibitor, and a diuretic simultaneously. In this scenario, the diuretic reduces plasma volume, the ACE inhibitor dilates the efferent arteriole, and the NSAID constricts the afferent arteriole. This combination causes a precipitous drop in the glomerular filtration rate (GFR), often leading to acute kidney injury (AKI). You can test your ability to identify these high-risk scenarios with our Pharmacology Practice Quizzes to ensure you’re ready for clinical rotations.
Hypersensitivity and the Aspirin-Exacerbated Respiratory Disease (AERD)
Some patients experience severe respiratory distress after taking these medications, a condition known as Samter’s Triad, which consists of asthma, nasal polyps, and aspirin sensitivity. This isn’t a typical IgE-mediated allergy but a result of the “leukotriene shift.” When the COX pathway is blocked, the available arachidonic acid is shunted toward the lipoxygenase (LOX) pathway. This leads to an overproduction of pro-inflammatory leukotrienes, which cause intense bronchoconstriction and mucus production. Recognizing this shift is vital for managing patients who present with sudden wheezing or nasal congestion after self-medicating for pain. It’s a classic example of how the NSAIDs mechanism of action and side effects are inextricably linked at the biochemical level.
Mastering NSAID Pharmacology for Board Exams
Success on the USMLE or NAPLEX depends on more than just recognizing drug names. It requires a deep understanding of the NSAIDs mechanism of action and side effects to solve complex clinical vignettes. You’ll often see questions that force you to prioritize one risk over another, such as choosing between GI protection and cardiovascular safety. To keep these diverse classes organized, many top-performing students rely on pharmacology study guides for nursing students to build a structured mental map of the COX pathway.
Drug-drug interactions are high-yield territory. NSAIDs can displace warfarin from albumin, which significantly increases the risk of hemorrhage. They also reduce the renal clearance of lithium and methotrexate. This leads to toxic accumulation of these narrow-therapeutic-index medications. Always look for these combinations in exam stems. Every agent in this class, except for aspirin, carries a mandatory FDA black box warning. These warnings highlight the risk of serious cardiovascular thrombotic events and life-threatening gastrointestinal events like bleeding and perforation. These risks can occur early in treatment and often without warning. For commercial drivers, ensuring they are both physically fit and technically proficient is a safety priority, which is why many turn to eastusatrucking.com for ongoing training and refresher courses.
Mnemonics for NSAID Side Effects
Using the “NSAID” mnemonic helps consolidate the diverse risks we’ve discussed. “N” stands for No urine, reminding you of the renal risks and potential for acute kidney injury. “S” reminds you of Systolic issues, covering hypertension and cardiovascular risks. “A” represents Asthma, specifically the leukotriene-mediated AERD. “I” is for Indigestion and GI bleeding, while “D” covers Dizziness or other CNS effects, which are critical safety considerations for tasks like operating a vehicle. For those in the Pacific Northwest, Seattle Driving Academy emphasizes that mental clarity is just as vital as technical skill when navigating the road. Differentiating propionic acid derivatives from acetic acid ones is easier when you group them by their suffixes and clinical niches. Visualizing the COX pathway isn’t just for the first year of school; it’s the key to long-term memory.
Exam Strategy: Clinical Case Integration
Identifying the “wrong” patient is half the battle in board questions. Avoid these drugs in patients with chronic kidney disease or those who’ve recently suffered a myocardial infarction. If an NSAID is absolutely necessary for a patient with high cardiovascular risk, naproxen is often the preferred choice due to its relatively lower thrombotic profile. For a rapid review of these clinical scenarios, PharmEDU High-Yield Video Vignettes provide a concise way to reinforce these concepts before your exam date. Mastering these patterns allows you to predict the correct answer before even reading the options.
Advancing Your Clinical Pharmacology Expertise
Navigating the complexities of drug classes shouldn’t feel like an administrative burden. We’ve analyzed how the NSAIDs mechanism of action and side effects stem from a logical molecular cascade, from the initial arachidonic acid substrate to the final physiological impact on the gastric mucosa and renal blood flow. This systematic approach transforms a list of facts into a functional clinical framework. Whether you’re differentiating between propionic acid derivatives or identifying a leukotriene shift, your ability to predict these outcomes is essential for patient safety and professional excellence. In a clinical setting, this excellence is often supported by community partners like Sage Creek Pharmacy, who prioritize patient well-being through personalized care and medication expertise.
To further solidify these concepts and prepare for your next career milestone, we invite you to leverage our specialized resources. Stop struggling with drug mechanisms. Join PharmEDU today for high-yield pharmacology review. Our platform features over 100 high-yield topics and mobile-compliant micro-learning segments designed by healthcare educators for board exam success. You don’t have to navigate these challenging scientific results alone. Your professional advancement is our priority, and we’re committed to providing the precision tools you need to succeed. Keep pushing forward; your dedication to clinical mastery makes a difference.
Frequently Asked Questions
Is acetaminophen (Tylenol) considered an NSAID?
No, acetaminophen isn’t categorized as an NSAID. While it effectively reduces pain and fever, it lacks the peripheral anti-inflammatory properties that define this drug class. This distinction is vital for understanding the NSAIDs mechanism of action and side effects, as acetaminophen’s lack of peripheral COX inhibition means it doesn’t carry the same gastric or anti-inflammatory risks.
Why do NSAIDs cause stomach ulcers?
Stomach ulcers occur because these drugs inhibit the COX-1 enzyme, which is responsible for producing cytoprotective prostaglandins. Prostaglandins like PGE2 and PGI2 maintain the gastric mucosal barrier by stimulating mucus and bicarbonate secretion. When these levels drop, the stomach lining is exposed to acidic damage, leading to erosions and eventual ulceration.
Can I take ibuprofen if I have high blood pressure?
Caution is required if you have hypertension. These medications can raise blood pressure by promoting sodium and water retention in the kidneys. They also block vasodilatory prostaglandins that normally help keep blood vessels open. Patients with established heart disease or uncontrolled hypertension should consult a provider before regular use to avoid cardiovascular strain. For those seeking professional guidance, AskMyDoc.ca provides virtual doctor appointments in Manitoba; read more.
Additionally, for those exploring alternative treatments for chronic pain that avoid the cardiovascular risks of NSAIDs, check out CMed to learn more about obtaining a medical marijuana card through an online evaluation.
What is the mechanism behind the “Triple Whammy” effect on kidneys?
The “Triple Whammy” happens when NSAIDs, diuretics, and ACE inhibitors are used together. Diuretics reduce overall blood volume, while ACE inhibitors dilate the efferent arteriole of the kidney. NSAIDs then constrict the afferent arteriole. This simultaneous reduction in pressure and volume causes a sudden drop in the glomerular filtration rate, often resulting in acute kidney failure.
How does aspirin differ from other NSAIDs in its mechanism?
Aspirin is unique because it irreversibly acetylates the COX enzyme active site. Most other agents are competitive inhibitors that eventually detach from the enzyme. Because aspirin’s bond is permanent, its antiplatelet effect lasts for the entire seven to ten day lifespan of the platelet, which is why it’s so effective for long-term cardiovascular protection.
What are the symptoms of NSAID-induced hypersensitivity?
Symptoms of NSAID-induced hypersensitivity often include sudden wheezing, shortness of breath, and nasal congestion. Some patients also develop skin rashes or facial swelling. These reactions are typically caused by a “leukotriene shift,” where blocking the COX pathway shunts arachidonic acid toward the production of pro-inflammatory leukotrienes, causing intense respiratory constriction.
Why are COX-2 inhibitors associated with higher cardiovascular risk?
Selective COX-2 inhibitors are associated with higher cardiovascular risk because they disrupt the balance of pro-thrombotic and anti-thrombotic factors. They inhibit prostacyclin, which prevents clotting and dilates vessels, but they don’t inhibit thromboxane A2. This imbalance creates an environment where blood is more likely to clot, increasing the risk of heart attack or stroke in vulnerable patients.
How long before surgery should a patient stop taking NSAIDs?
Most patients are advised to stop taking reversible NSAIDs like ibuprofen or naproxen about two to three days before a procedure. For aspirin, the window is longer, usually seven to ten days, because of its irreversible effect on platelets. Always follow specific surgical guidelines, as the timing can vary based on the type of surgery and the patient’s individual bleeding risk profile.