Antifungal Agents Study Guide: High-Yield Pharmacology for 2026
Did you know that fungal infections now contribute to over 3.8 million deaths annually, while resistance rates for common treatments like voriconazole have climbed to 14.6%? These statistics represent the increasing clinical complexity you’ll face on your upcoming exams, making a comprehensive antifungal agents study guide an essential tool for your success. It’s completely normal to feel overwhelmed by drug names that sound nearly identical or to struggle with the distinct ways various agents inhibit ergosterol. Most students find themselves circling through mechanisms of action until the details blur together, making it difficult to prioritize the most relevant information.
This guide provides the logical structure you need to categorize these medications with professional precision. We’ll move beyond rote memorization to help you master drug classifications, understand the severity of side effects like nephrotoxicity, and integrate the 2026 IDSA guideline updates for aspergillosis. You’ll gain a clear framework for identifying high-yield clinical pearls and the confidence to tackle the most challenging pharmacology board questions with ease.
Key Takeaways
- Differentiate between ergosterol disruptors and cell wall inhibitors by focusing on their specific fungal cell targets rather than rote memorization.
- Identify high-yield toxicities, specifically nephrotoxicity, hepatotoxicity, and bone marrow suppression, to accurately answer clinical board vignettes.
- Utilize this antifungal agents study guide to master drug suffixes and classification frameworks for rapid identification during time-pressured exams.
- Understand the critical role of CYP450 inhibition in the azole class to predict and manage complex drug-drug interactions.
- Map adverse reactions directly back to their biochemical mechanisms to ensure long-term retention of pharmacological principles.
Classification of Antifungal Agents by Mechanism of Action
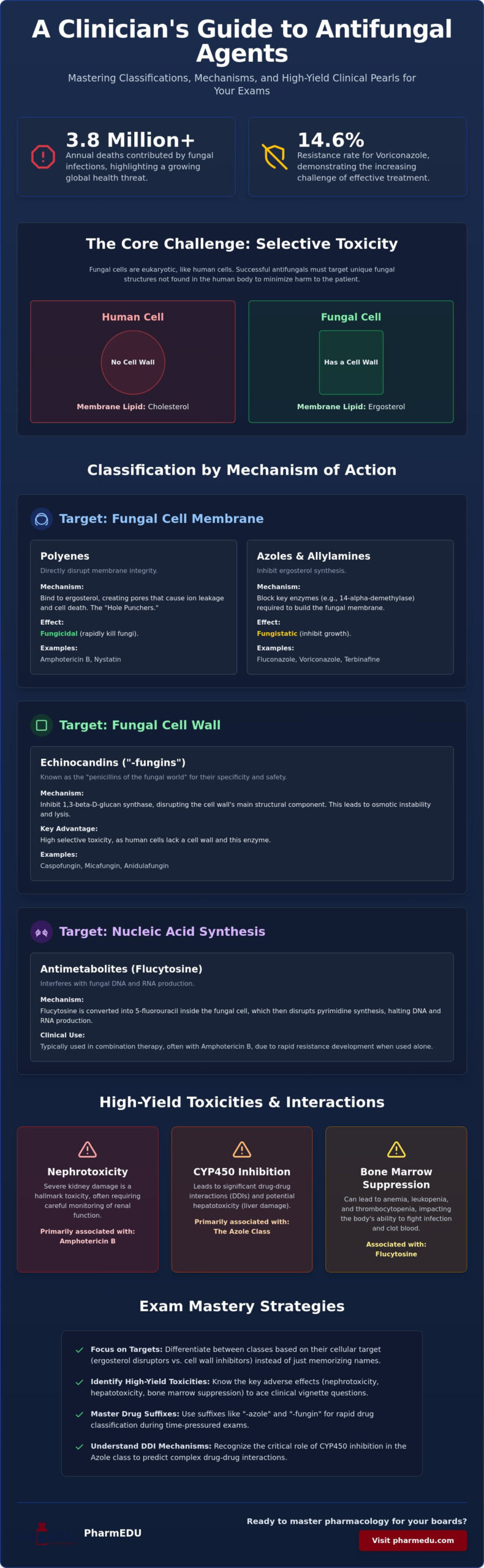
Fungal cells present a unique pharmacological challenge because they are eukaryotic, just like human cells. This biological similarity makes achieving selective toxicity, which is the ability to kill the pathogen without harming the host, considerably harder than it is with bacteria. To succeed on your boards, you must recognize that most successful therapies target the specific differences in lipid composition or structural components that aren’t found in human physiology. This antifungal agents study guide categorizes these drugs into four primary groups based on where they strike the fungal cell to help you organize your clinical knowledge.
Group 1 consists of Polyenes, which physically disrupt the membrane. Group 2 includes Azoles and Allylamines; these agents stop the synthesis of essential membrane components. Group 3 features Echinocandins, which target the cell wall itself. Finally, Group 4 contains antimetabolites like Flucytosine that interfere with nucleic acid production. Understanding these distinctions is the first step toward mastering the complex treatment algorithms used for the 3.8 million people affected by serious fungal infections annually.
Targeting the Fungal Cell Membrane
Ergosterol is the “Achilles heel” of fungal pharmacology. While human cell membranes rely on cholesterol for fluidity and integrity, fungi utilize ergosterol. This distinction allows an Antifungal medication to selectively target the pathogen. However, the methods of attack differ significantly between classes. You’ll find that Polyenes, such as Amphotericin B and Nystatin, act like molecular “hole punches.” They bind directly to existing ergosterol, creating transmembrane pores that cause ion leakage and rapid cell death.
In contrast, Azoles and Allylamines are synthesis inhibitors rather than direct disruptors. Azoles, including Fluconazole and Voriconazole, block the enzyme 14-alpha-demethylase. Allylamines, such as Terbinafine, inhibit squalene epoxidase. Both prevent the fungus from building its membrane in the first place. It’s helpful to remember that Polyenes are generally fungicidal due to direct damage, whereas Azoles are often fungistatic, merely halting growth until the immune system can respond.
Targeting the Fungal Cell Wall
The fungal cell wall is an even more specific target than the membrane because human cells lack a cell wall entirely. This structure relies on beta-glucan polymers for its mechanical strength and structural integrity. Echinocandins, often referred to as the “fungins” (specifically Caspofungin, Micafungin, and Anidulafungin), inhibit the enzyme 1,3-beta-D-glucan synthase.
Because humans don’t have this enzyme or a cell wall, these inhibitors typically have fewer systemic side effects than membrane disruptors. They’ve become the preferred choice for invasive candidiasis, especially as resistance rates for older drugs continue to climb. When using this antifungal agents study guide, think of Echinocandins as the “penicillins of the fungal world.” They cause osmotic instability and lysis by compromising the outer shell, providing a highly effective and relatively safe therapeutic window for critically ill patients.
The Ergosterol Disruptors: Polyenes and Azoles
When you encounter a board question regarding systemic fungal infections, your mind should immediately go to the agents that target ergosterol. This lipid is the primary component of the fungal cell membrane, serving a role similar to cholesterol in humans. This antifungal agents study guide focuses on the two heavy hitters of membrane disruption: the Polyenes and the Azoles. While both target the same membrane integrity, their methods are fundamentally different. One acts as a physical disruptor, while the other functions as a metabolic inhibitor. Understanding this distinction is vital for predicting clinical outcomes and side effect profiles.
Polyenes: The “Shake and Bake” Drugs
Amphotericin B is often called “Ampho-terrible” by clinicians due to its notorious toxicity profile. Polyenes function by binding to ergosterol and creating transmembrane pores that allow the leakage of essential electrolytes, leading to rapid cell death. This direct physical damage makes them potently fungicidal. However, because Amphotericin B can also bind to human cholesterol to a lesser degree, it often causes severe nephrotoxicity. You’ll likely see questions about “Shake and Bake” reactions, which refer to the fever and chills that occur during infusion. To mitigate these risks, modern medicine utilizes liposomal formulations. These lipid-based delivery systems “hide” the drug from human kidneys, allowing for higher doses with significantly less renal damage.
Nystatin is another polyene you must recognize, though its use is strictly limited. It’s too toxic for systemic administration. Instead, it’s used topically or as a “swish and swallow” preparation for oral candidiasis. Since it isn’t absorbed by the GI tract, it remains safe for local treatment. Mastery of these nuances is easier with Interactive Pharmacology Flashcards that help you drill these class-specific side effects and clinical applications.
Azoles: The Cytochrome P450 Interaction Giants
Azoles represent a massive class of drugs that inhibit the enzyme 14-alpha-demethylase, which converts lanosterol into ergosterol. By halting this synthesis, they leave the fungus with a leaky, dysfunctional membrane. You should categorize these into two groups: the older Imidazoles (like Ketoconazole) and the newer Triazoles (like Fluconazole and Voriconazole). The Triazoles are the current standard for systemic therapy because they have a higher affinity for fungal enzymes than human ones. However, all azoles are notorious for inhibiting the human Cytochrome P450 system. This leads to a mountain of drug-drug interactions that you must account for in clinical practice.
Specific drug profiles often appear on exams. Fluconazole is the go-to for Candida and cryptococcal meningitis because it crosses the blood-brain barrier effectively. Voriconazole is the treatment of choice for invasive aspergillosis, but it carries a unique side effect: transient visual disturbances or “shimmering lights.” Ketoconazole is rarely used systemically today because it inhibits human steroid synthesis, leading to anti-androgenic effects like gynecomastia. As noted in recent literature on Antifungal Agents, keeping track of these varying spectra of activity is essential as resistance rates continue to climb, with voriconazole resistance now estimated at 14.6% globally.
Cell Wall and DNA Synthesis Inhibitors: Echinocandins and Flucytosine
While previous sections of this antifungal agents study guide focused on the cell membrane, we must now turn our attention to the drugs that attack the structural integrity of the cell wall and the machinery of genetic replication. These agents often provide a safer therapeutic window or essential synergistic effects for life-threatening infections. By targeting components like beta-glucan or specific fungal enzymes, these medications offer precision that older, more toxic systemic treatments sometimes lack.
The “Fungins” and the Beta-Glucan Target
Echinocandins represent the newest major class of antifungals in the clinical arsenal. You can easily identify these agents by their “-fungin” suffix: Caspofungin, Micafungin, and Anidulafungin. Their mechanism is highly specific and elegant. They inhibit the synthesis of 1,3-beta-D-glucan, which is a critical structural component of the fungal cell wall. Because human cells don’t possess a cell wall, these drugs are exceptionally well-tolerated with a very low incidence of systemic toxicity.
In the ICU setting, you’ll frequently see Echinocandins used as first-line empirical therapy for invasive candidiasis and candidemia. They’re particularly valuable for critically ill patients because they don’t require renal dose adjustments. This pharmacokinetic profile allows clinicians to maintain steady therapeutic levels without the constant fear of exacerbating acute kidney injury. When studying for your boards, remember that these are the “heavy hitters” for Candida species that have developed resistance to azoles.
Antimetabolites and Allylamines
Flucytosine is a unique antimetabolite that functions as a prodrug. Fungal cells take it up and convert it into 5-fluorouracil via the enzyme cytosine deaminase. Human cells lack this specific enzyme, which provides the necessary selective toxicity. Once converted, the molecule interferes with both DNA and RNA synthesis. You’ll rarely see Flucytosine used as a monotherapy because resistance develops rapidly. Instead, it’s the classic partner for Amphotericin B in treating cryptococcal meningitis. This synergy is a high-yield exam topic; the polyene “opens the door” in the membrane, allowing Flucytosine to enter and halt replication. However, you must monitor patients for bone marrow suppression, which is its most significant adverse effect.
Terbinafine, an allylamine, takes a different approach by inhibiting squalene epoxidase. This leads to a toxic accumulation of squalene within the fungal cell while simultaneously preventing ergosterol synthesis. Clinically, it’s the gold standard for onychomycosis. It’s highly lipophilic and keratophilic, meaning it concentrates heavily in the skin and nails. This unique accumulation allows it to remain effective long after the patient finishes their course of treatment, making it ideal for stubborn dermatophyte infections. Utilizing an antifungal agents study guide to contrast these specific tissue distributions will help you distinguish between systemic and localized treatment options during clinical vignettes.
While medical students focus on the physiological aspects of skin health, those interested in the artistic side of skin application can check out Face Painting Course Online for professional training.
High-Yield Clinical Pearls and Adverse Reactions
Mastering the toxicities of these medications is as important as knowing their mechanisms. In this antifungal agents study guide, we categorize the “Big Three” adverse reactions: nephrotoxicity, hepatotoxicity, and bone marrow suppression. While you’ve already learned how these drugs strike the fungal cell, clinical success requires knowing how they affect the human host and how to monitor for those failures in a professional setting. Recognizing these patterns allows you to anticipate complications before they become life-threatening.
Managing the “Ampho-Terrible” Profile
Amphotericin B remains the primary culprit for drug-induced renal damage in the antifungal category. It causes both vasoconstriction of the afferent arterioles and direct tubular damage. To protect the patient’s kidneys, clinical protocols typically require a 1-liter saline bolus before infusion to maintain renal perfusion. You must also monitor potassium and magnesium levels daily. The drug often causes a “wasting” effect in the distal tubule, leading to severe hypokalemia and hypomagnesemia that require aggressive supplementation.
Infusion-related reactions are equally common. Patients often experience fever, chills, and rigors, which is why pre-medication is a standard of care. Nurses often administer acetaminophen, diphenhydramine, and sometimes hydrocortisone or meperidine to mitigate these “shake and bake” symptoms. If a board question asks about the safest systemic formulation, always choose the liposomal variant, as it significantly reduces the risk of nephrotoxicity compared to the older deoxycholate version.
Azole Side Effects and Monitoring
Azoles are the undisputed giants of drug-drug interactions. Because they inhibit various Cytochrome P450 enzymes, particularly CYP3A4, they slow the metabolism of many common medications. If a patient is on Warfarin, their INR will likely skyrocket. If they take Statins, they risk developing rhabdomyolysis. Beyond these interactions, hepatotoxicity is a class-wide concern. You should monitor Liver Function Tests (LFTs) regularly and consider discontinuing therapy if transaminases exceed three times the upper limit of normal. Test your ability to spot these complex interactions with our Pharmacology Practice Quizzes.
Cardiovascular and endocrine concerns also play a role in exam vignettes. Fluconazole and Voriconazole are known to cause QT prolongation, necessitating baseline and periodic EKG monitoring. Regarding pregnancy, most azoles are considered teratogenic and are generally avoided, especially during the first trimester. Griseofulvin is particularly notorious for its teratogenic potential and its ability to induce CYP450 enzymes, which is the opposite of the azole effect. For systemic infections in pregnant patients, Amphotericin B is often the safest choice despite its significant renal risks.
Mastery Strategies: How to Study Antifungals for Boards
Memorizing every antifungal drug is a recipe for burnout. Instead, professional students use a structured antifungal agents study guide approach that prioritizes logic over rote memorization. The first step involves mastering common suffixes. When you see “-azole,” you immediately know you’re dealing with ergosterol synthesis inhibition and potential CYP450 interactions. When you see “-fungin,” your mind should pivot to cell wall synthesis and the ICU setting. These linguistic shortcuts allow you to categorize the majority of exam questions in seconds.
The second step is mapping side effects directly back to the drug’s mechanism. Don’t just remember that Amphotericin B causes kidney damage; remember it’s because the drug’s affinity for ergosterol occasionally crosses over to human cholesterol. This conceptual link makes the information “sticky.” You’ll find that once the mechanism is clear, the adverse reactions become predictable rather than random facts to be memorized. This logical flow is what separates top performers from those who struggle with similar-sounding names.
Utilizing PharmEDU for Exam Success
Visual and auditory learners often struggle with the dry text of traditional pharmacology resources. Our High-Yield Video Vignettes simplify complex antifungal pathways by using clinical scenarios that mirror what you’ll see on the boards. These short, focused videos help you visualize the “hole-punching” action of polyenes or the enzymatic blockade of azoles, ensuring the concepts remain vivid during high-pressure testing. They turn abstract biochemistry into concrete clinical images.
For long-term retention, consistency is key. Leveraging Interactive Pharmacology Flashcards allows you to use spaced repetition to drill high-yield facts during short study breaks. If you’re looking for a broader framework to organize your entire semester, check out The Ultimate Pharmacology Study Guide for Nursing Students in 2026. Combining these resources ensures you aren’t just passing the test, but building a foundation for safe clinical practice.
Active Recall and Case Studies
The final phase of mastery is application. You can’t truly know if you’ve mastered this antifungal agents study guide until you apply it to Clinical Case Studies. These scenarios force you to choose the best agent for a patient with cryptococcal meningitis or a transplant recipient facing invasive aspergillosis. This mimics the actual decision-making process required by board examiners, where you must weigh the benefits against the risks of toxicity.
Simulating board conditions with Pharmacology Practice Quizzes is the best way to identify your weak spots. Focus your study schedule on high-weight exam topics like the systemic azoles and the “fungins.” By testing yourself early and often, you build the stamina and speed necessary for success. It’s better to discover a gap in your knowledge during a practice session than during the actual exam. For students preparing for Indian competitive exams, PYQKosh offers an excellent way to practice topic-wise and subtopic-wise previous year questions. Ultimately, the goal isn’t to read the most pages, but to correctly answer the most questions.
Elevate Your Pharmacology Mastery
Mastering the complexities of fungal therapy requires more than just memorizing a list of drugs; it demands a deep understanding of biochemical targets and clinical safety profiles. By categorizing agents by their mechanism of action, you’ve transitioned from simple recognition to professional-level analysis. You now understand how to distinguish between membrane disruptors like Amphotericin B and cell wall inhibitors like the “fungins,” while staying vigilant for high-yield side effects such as QT prolongation and bone marrow suppression. This antifungal agents study guide serves as your roadmap for navigating the evolving landscape of 2026 clinical guidelines.
To truly solidify this knowledge and ensure you’re ready for exam day, you need tools designed for the modern medical professional. PharmEDU provides over 100 high-yield pharmacology topics through mobile-compliant micro-learning segments that fit into your busy schedule. You can access expert-led video vignettes and interactive quizzes that turn passive reading into active recall. Master Antifungals and Pass Your Boards with PharmEDU today to gain the confidence you need. You’ve got the drive to succeed, and we’re here to provide the precision tools to get you there.
Frequently Asked Questions
What is the most common side effect of Amphotericin B?
The most common side effects of Amphotericin B are acute infusion-related reactions, often described as “shake and bake” symptoms, and dose-limiting nephrotoxicity. These reactions occur because the drug triggers a systemic inflammatory response during administration. To manage these, clinicians often pre-medicate with acetaminophen or antihistamines. Long-term use requires careful monitoring of renal function and electrolyte levels to prevent permanent kidney damage.
How do Azole antifungals interact with other medications?
Azole antifungals interact with other medications primarily by inhibiting the Cytochrome P450 enzyme system, specifically the CYP3A4 isoenzyme. This inhibition slows the metabolism of co-administered drugs like warfarin, statins, and certain anticonvulsants, leading to potentially toxic serum levels. It’s vital for healthcare providers to perform a thorough drug-interaction screen whenever an azole is added to a patient’s treatment regimen.
Which antifungal agent is used specifically for nail infections?
Terbinafine is the primary antifungal agent used for treating onychomycosis, or fungal nail infections. This medication is highly lipophilic and keratophilic, which means it concentrates in the skin, hair, and nail beds for extended periods. This antifungal agents study guide highlights that Terbinafine’s ability to remain in the nail tissue even after the treatment course ends makes it the preferred choice for stubborn dermatophyte infections.
Can Echinocandins be used to treat Cryptococcal meningitis?
No, Echinocandins cannot be used to treat Cryptococcal meningitis because they lack significant activity against Cryptococcus neoformans. This fungus has a unique cell wall composition that doesn’t rely as heavily on the 1,3-beta-D-glucan synthesis pathway targeted by the “fungins.” Instead, clinicians typically utilize a combination of Amphotericin B and Flucytosine as the standard induction therapy for central nervous system infections.
Why is Flucytosine rarely used as a monotherapy?
Flucytosine is rarely used as a monotherapy because fungal pathogens develop resistance to it extremely quickly when it’s used alone. To prevent this, it’s almost always paired with Amphotericin B, which helps the Flucytosine penetrate the fungal cell membrane. This combination therapy is particularly high-yield for treating systemic infections like cryptococcosis where synergy is essential for effective clearance of the pathogen.
What are the primary differences between Type 1 and Type 2 fungal cell targets?
The primary difference between fungal cell targets involves the distinction between the cell membrane and the cell wall. Type 1 targets focus on the cell membrane, specifically ergosterol, and are addressed by polyenes and azoles. Type 2 targets involve the cell wall, primarily beta-glucans, which are the focus of echinocandins. Understanding these structural differences is a core component of any comprehensive antifungal agents study guide.
Is Fluconazole safe to use during pregnancy?
Fluconazole is generally avoided during pregnancy, particularly in high doses or during the first trimester, due to its potential teratogenic effects. While a single low dose for vaginal candidiasis is sometimes considered, systemic use has been linked to specific congenital malformations. Most clinical guidelines recommend safer alternatives like topical nystatin or, for severe infections, Amphotericin B, which doesn’t cross the placenta as readily.
How do liposomal formulations of antifungals differ from standard versions?
Liposomal formulations of antifungals differ from standard versions by encapsulating the active drug within a lipid bilayer. This delivery system allows the drug to stay in the blood longer and reduces its exposure to the renal tubules, which significantly lowers the risk of nephrotoxicity. While more expensive, these formulations permit higher dosing for life-threatening infections while protecting the patient’s kidney function.