Pharmacology of Hypertension Management: High-Yield Study Guide for 2026
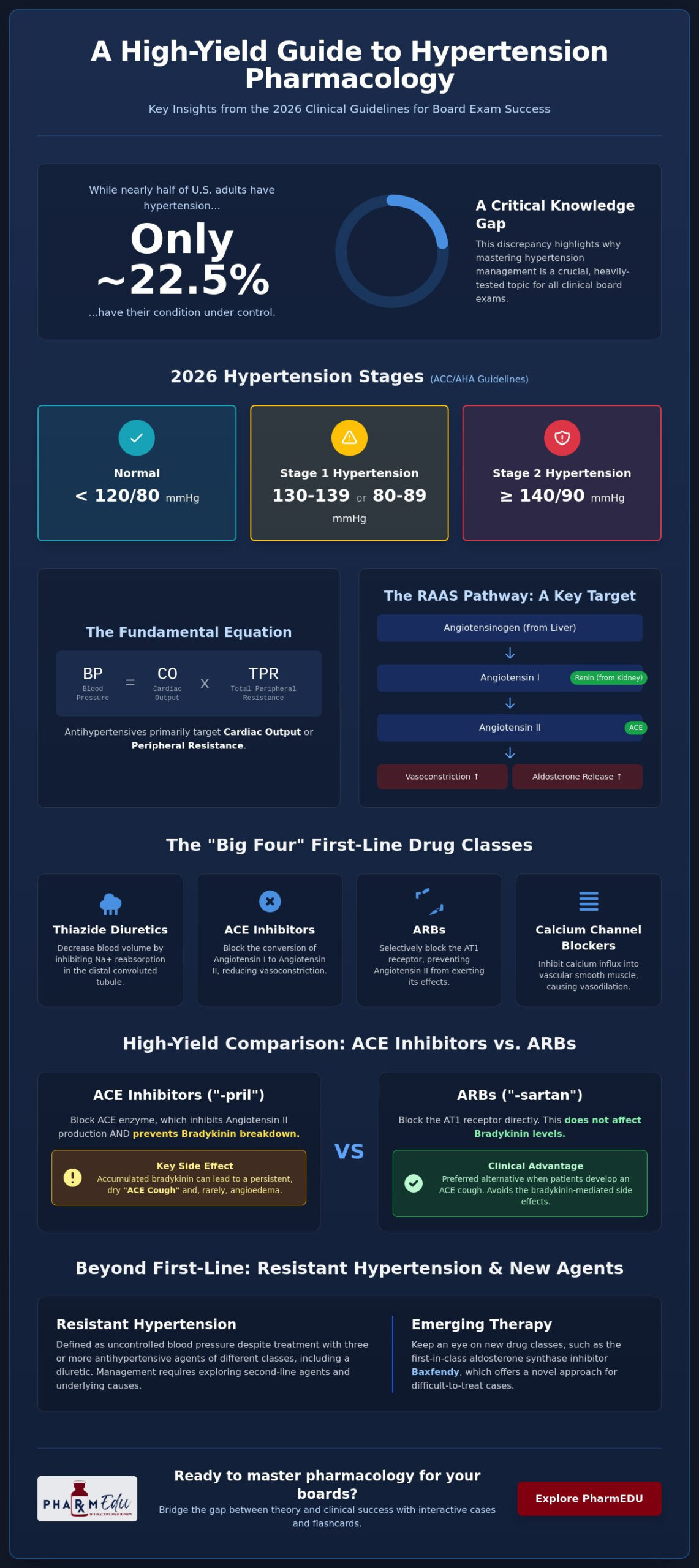
Did you know that while nearly half of U.S. adults live with hypertension, only about 22.5% actually have their blood pressure under control? It’s a staggering reality that underscores why the pharmacology of hypertension management remains one of the most heavily tested topics on board exams. We understand that the sheer volume of drug names, contraindications, and side effect profiles can feel overwhelming. Distinguishing between first-line agents and second-line treatments shouldn’t feel like a guessing game during a high-stakes clinical case.
This guide provides the high-yield framework you need to move past rote memorization and toward clinical mastery. You’ll learn to match drug mechanisms to specific patient comorbidities using the latest 2025 ACC/AHA guidelines. We’ll break down the primary drug classes, explore the clinical nuances of the new PREVENT equations, and introduce emerging therapies like the first-in-class aldosterone synthase inhibitor, Baxfendy. By the end of this study guide, you’ll have the confidence to navigate complex pharmacotherapy questions with precision and ease.
Key Takeaways
- Identify the latest 2026 clinical thresholds for hypertension and the specific physiological factors, such as total peripheral resistance, that guide treatment selection.
- Master the “Big Four” first-line drug classes and their comparative efficacy across diverse patient demographics to excel in the pharmacology of hypertension management.
- Define resistant hypertension and explore the evolving role of second-line agents, including the latest first-in-class aldosterone synthase inhibitors.
- Recognize high-yield contraindications and electrolyte imbalances to avoid common board exam traps regarding drug-drug interactions and pregnancy.
- Learn how to leverage interactive flashcards and clinical case studies to bridge the gap between theoretical knowledge and board-style question success.
Core Principles of Pharmacotherapy for Hypertension Management
Managing blood pressure requires a deep understanding of the physiological variables that maintain systemic perfusion. In the pharmacology of hypertension management, we focus on the fundamental equation where blood pressure equals cardiac output multiplied by total peripheral resistance. Effective treatment hinges on identifying whether a patient’s elevation stems from increased heart rate, excessive stroke volume, or heightened vascular tone. According to the 2025 ACC/AHA guidelines, which remain the clinical standard for 2026, normal blood pressure is defined as less than 120/80 mmHg. Stage 1 hypertension is classified as 130 to 139 systolic or 80 to 89 diastolic, while Stage 2 begins at 140/90 mmHg or higher.
The decision to initiate pharmacotherapy depends heavily on a patient’s total cardiovascular risk profile. For individuals in Stage 2, medication is recommended regardless of other factors. However, for those in Stage 1, clinicians now use the PREVENT equations to estimate 10-year cardiovascular disease risk. If that risk is 7.5% or higher, or if the patient has existing clinical cardiovascular disease, diabetes, or chronic kidney disease, immediate pharmacological intervention is necessary. For lower-risk Stage 1 patients, a three to six month trial of lifestyle modifications is typically the first step before reassessing the need for drugs.
The RAAS Pathway and Blood Pressure Regulation
The Renin-Angiotensin-Aldosterone System (RAAS) serves as a primary target for many modern therapies. The process begins in the kidneys, where the release of renin converts angiotensinogen into angiotensin I. This inactive precursor then travels through the vasculature to be activated. Angiotensin-converting enzyme (ACE) catalyzes the conversion of angiotensin I into angiotensin II, which is a potent vasoconstrictor that also stimulates the release of aldosterone. By interrupting this pathway, we can effectively reduce systemic vascular resistance and decrease sodium and water retention, which are core goals in the pharmacology of hypertension management.
Hemodynamic Goals of Antihypertensive Agents
Antihypertensive agents typically fall into two categories based on their hemodynamic effects: those that reduce cardiac output and those that lower peripheral resistance. Cardio-inhibitors focus on decreasing heart rate and stroke volume to take the pressure off the arterial walls. Conversely, vasodilators and diuretics aim to reduce afterload and blood volume. A mastery of pharmacology fundamentals is essential to understand how these Antihypertensive Medications interact with the body’s compensatory mechanisms. Reducing afterload is particularly critical in chronic management, as it prevents the long-term cardiac remodeling and end-organ damage associated with untreated Stage 2 hypertension.
First-Line Antihypertensive Drug Classes: Mechanisms and Indications
The 2026 treatment algorithms continue to prioritize the “Big Four” drug classes as the foundation for the pharmacology of hypertension management. These include thiazide or thiazide-like diuretics, angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), and long-acting dihydropyridine calcium channel blockers (CCBs). Selecting the appropriate initial agent isn’t just about lowering numbers; it’s about matching the drug’s molecular mechanism to the patient’s specific clinical phenotype. While most patients achieve control through these classes, the WHO Hypertension Treatment Guidelines emphasize that the choice should also account for cardiovascular risk and potential side effect profiles.
ACE Inhibitors vs. Angiotensin II Receptor Blockers (ARBs)
Understanding ACE inhibitors is essential for any board candidate. These agents inhibit the enzyme responsible for converting Angiotensin I to the potent vasoconstrictor Angiotensin II. However, they also prevent the breakdown of bradykinin. This accumulation of bradykinin often leads to the infamous “ACE cough” or, more seriously, angioedema. When these side effects occur, ARBs are the preferred alternative because they block the AT1 receptor directly without affecting bradykinin levels. Clinical scenarios like diabetes mellitus and chronic kidney disease (CKD) make RAAS inhibition mandatory due to their proven renoprotective effects and ability to reduce albuminuria.
Calcium Channel Blockers and Thiazide Diuretics
Calcium channel blockers are divided into two distinct sub-groups. Dihydropyridines, like amlodipine, primarily cause peripheral vasodilation and are excellent for reducing systemic vascular resistance. Non-dihydropyridines, such as verapamil and diltiazem, have more pronounced cardiac effects and are used when rate control is also required. A high-yield fact for clinical rotations is that CCBs and thiazides are often more effective as initial monotherapy for patients of African descent compared to RAAS inhibitors. Thiazide diuretics, specifically chlorthalidone or hydrochlorothiazide, work in the distal convoluted tubule by inhibiting the Na+/Cl- symporter. This results in increased sodium excretion, though clinicians must monitor for electrolyte shifts like hypokalemia and hypercalcemia.
Mastering the nuances between these classes requires more than just reading a list of names. If you find the comparative efficacy of these drugs confusing, our Interactive Pharmacology Flashcards can help you solidify these distinctions through active recall. These tools are designed to bridge the gap between textbook theory and the high-pressure environment of board-style clinical case questions, ensuring you understand the pharmacology of hypertension management at a professional level.
Second-Line Agents and Management of Resistant Hypertension
When the “Big Four” drug classes fail to achieve target blood pressure, clinicians must pivot to second-line agents. Resistant hypertension is strictly defined as blood pressure that remains above the 130/80 mmHg goal despite the use of three or more antihypertensive medications of different classes, one of which must be a diuretic, all at maximum tolerated doses. In the modern pharmacology of hypertension management, this scenario often triggers the addition of a fourth-line agent, typically an aldosterone antagonist like spironolactone. Spironolactone excels in resistant cases by blocking the mineralocorticoid receptor, though it requires careful monitoring for hyperkalemia and gynecomastia.
The therapeutic landscape for resistant cases is expanding rapidly. The FDA’s May 2026 approval of Baxfendy (baxdrostat), a first-in-class aldosterone synthase inhibitor, provides a new mechanism for patients whose blood pressure isn’t adequately controlled. This drug offers a targeted approach to lowering aldosterone levels without some of the off-target effects seen with older antagonists. Mastery of these nuances is what separates a standard practitioner from a board-ready expert.
Beta-Blockers: Selective vs. Non-Selective
Beta-blockers have transitioned from first-line monotherapy to specialized roles in the pharmacology of hypertension management. We categorize them based on their receptor affinity. B1-selective agents, such as metoprolol and atenolol, primarily target the heart to reduce cardiac output and renin release. Non-selective agents like propranolol block both B1 and B2 receptors, which can lead to bronchospasm. This makes them strictly contraindicated in patients with asthma. Mixed alpha and beta blockers, specifically carvedilol and labetalol, are indispensable in managing hypertension comorbid with heart failure or during pregnancy. Clinicians must also remain cautious when using these in patients with peripheral vascular disease, as B2 blockade can worsen vasospasm.
Centrally Acting Agents and Direct Vasodilators
Centrally acting agents like clonidine and methyldopa work by stimulating alpha-2 receptors in the brainstem, effectively reducing sympathetic outflow. Methyldopa remains a high-yield favorite for pregnancy-related hypertension due to its established safety profile and long-term data. Direct vasodilators, including hydralazine and minoxidil, are powerful but come with significant compensatory responses. They often trigger reflex tachycardia and sodium retention; this usually necessitates the co-administration of a beta-blocker and a loop diuretic. In the acute setting of a hypertensive crisis, clinicians rely on nitroprusside for its rapid onset, though they must monitor for cyanide toxicity. Fenoldopam, a dopamine D1 receptor agonist, serves as an alternative that maintains renal perfusion while lowering systemic pressure.
High-Yield Board Review: Side Effects, Traps, and Contraindications
Mastering the pharmacology of hypertension management requires more than just knowing how drugs work; you must anticipate how they fail or cause harm in specific patient populations. Board exams frequently test your ability to recognize these “traps” through clinical vignettes where a patient’s comorbid condition makes a standard treatment dangerous. Electrolyte management is a perennial favorite for examiners. You should remember that RAAS inhibitors and potassium-sparing diuretics promote hyperkalemia, while thiazides and loop diuretics typically lead to hypokalemia. Distinguishing these shifts is vital for managing patients on multi-drug regimens.
Teratogenicity is another non-negotiable topic. ACE inhibitors, ARBs, and direct renin inhibitors are strictly contraindicated in pregnancy due to the risk of fetal renal dysgenesis and skull hypoplasia. If a clinical case involves a hypertensive pregnant patient, your mind should immediately pivot to methyldopa, labetalol, or nifedipine. Additionally, metabolic profiles can be significantly altered by therapy. Thiazide diuretics are known for the “Hyper” side effects: hyperuricemia (triggering gout), hypercalcemia, and hyperglycemia. Understanding these nuances ensures you don’t inadvertently worsen a patient’s secondary condition while treating their primary hypertension.
Patient-Specific Contraindications
A classic board question involves a patient with bilateral renal artery stenosis who develops acute renal failure after starting an ACE inhibitor. This occurs because these patients rely on angiotensin II-mediated efferent arteriolar vasoconstriction to maintain their glomerular filtration rate. When you remove that vasoconstriction, the GFR plummets. Another high-yield scenario involves diabetic patients on beta-blockers. These agents can mask the sympathetic symptoms of hypoglycemia, such as tachycardia and tremors, leaving only diaphoresis as a clinical clue. This “masking” effect makes beta-blockers a cautious choice for those with poorly controlled blood glucose.
Drug Class Specific Adverse Effects
Specific classes carry unique “signature” side effects that are frequently tested. Calcium channel blockers, particularly dihydropyridines like amlodipine, often cause dose-dependent peripheral edema and, less commonly, gingival hyperplasia. If a vignette mentions a patient with new-onset joint pain, a malar rash, and positive anti-histone antibodies while taking hydralazine, you are looking at drug-induced lupus erythematosus. Alpha-1 antagonists, used for both hypertension and BPH, are notorious for first-dose syncope. To minimize this risk, clinicians advise patients to take their initial dose at bedtime. Additionally, for those managing the long-term impact of therapy on sexual health, you can visit ED Health Clinic for specialized and confidential support. These details are the difference between a passing score and true mastery.
Identifying these clinical traps under pressure is a skill that requires practice. You can refine your diagnostic accuracy by working through our Pharmacology Practice Quizzes, which are specifically designed to mirror the complexity of board-style side effect questions. By testing yourself on these high-yield contraindications now, you ensure that these common exam pitfalls don’t catch you off guard on test day.
Mastering Hypertension Pharmacology with PharmEDU
The pharmacology of hypertension management is a vast field where guidelines and drug approvals shift rapidly. Relying solely on static textbooks often leaves students ill-prepared for the dynamic nature of 2026 clinical practice. PharmEDU bridges this gap by transforming dense pharmacological data into actionable, high-yield knowledge. Our platform is built on the premise that true mastery comes from understanding mechanisms rather than simply memorizing lists. Through High-Yield Video Vignettes, we simplify the most complex drug pathways, such as the intricacies of aldosterone synthase inhibition or the specific hemodynamic effects of mixed alpha and beta blockers.
Active recall is the cornerstone of effective board preparation. Our Interactive Pharmacology Flashcards allow students to master drug names, classes, and side effect profiles through proven spaced repetition techniques. When it’s time to put that knowledge to the test, our Pharmacology Practice Quizzes are specifically engineered to mimic the question styles found on the NAPLEX and USMLE. These aren’t just simple recall questions; they are Clinical Case Studies that require you to apply the pharmacology of hypertension management to real-world scenarios, such as managing a patient with Stage 2 hypertension and comorbid chronic kidney disease.
The PharmEDU Learning Methodology
We recognize that medical and nursing students are often balancing clinical rotations with heavy study schedules. That’s why our methodology focuses on micro-learning segments that fit into a busy day. These focused bursts of information help you retain critical details about drug-drug interactions and patient-specific contraindications without the burnout associated with long lectures. Prepare for your boards with a comprehensive pharmacy review platform that prioritizes efficiency and scientific accuracy over academic fluff.
Subscription Benefits for Students and Institutions
Whether you’re an individual learner or part of a larger academic program, our platform scales to meet your needs. A PharmEDU Monthly or Annual Subscription provides unlimited access to over 100 pharmacology topics, including the latest 2026 clinical guidelines and drug approvals. We also offer Institutional Platform Licenses for universities and pharmacy schools looking to integrate high-quality digital content into their core curricula. Don’t let an overwhelming number of drug classes hinder your academic progress. Excel in your pharmacology coursework with PharmEDU and gain the confidence needed to succeed on your board exams and in your future clinical career.
Advancing Toward Clinical Excellence in Hypertension Care
Navigating the complex landscape of antihypertensive therapy requires a structured approach that balances physiological targets with patient-specific comorbidities. You’ve now explored the core principles of the latest guidelines, the nuances of the “Big Four” first-line drug classes, and the emerging pharmacological solutions for resistant cases. Success on your upcoming board exams depends on your ability to identify clinical traps, such as electrolyte imbalances or pregnancy contraindications, while maintaining a clear understanding of systemic hemodynamics.
Mastering the pharmacology of hypertension management is a journey of continuous refinement. To ensure you’re fully prepared for test day and clinical practice, leverage a platform that evolves alongside the latest medical standards. With over 100 high-yield pharmacology topics, expert-led video vignettes for visual learners, and interactive flashcards paired with board-style quizzes, we provide the tools necessary to bridge the gap between theory and professional success. Start your high-yield pharmacology review with PharmEDU today and turn confusing drug classes into your greatest clinical strength. We’re here to support your growth every step of the way toward becoming a confident, expert practitioner.
Frequently Asked Questions
What is the first-line treatment for hypertension in patients with diabetes?
Angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs) are the preferred first-line agents for patients with diabetes. These drugs provide essential renoprotection by reducing intraglomerular pressure and slowing the progression of diabetic nephropathy. While other classes like thiazides or calcium channel blockers are effective, the specific vascular benefits of RAAS inhibition make them the standard of care for this patient population.
Why are ACE inhibitors contraindicated in pregnancy?
ACE inhibitors are strictly avoided in pregnancy because they are known teratogens that interfere with the fetal renin-angiotensin system. This system is vital for normal kidney development in the womb. Exposure during the second and third trimesters can lead to fetal renal failure, oligohydramnios, and skeletal deformities such as skull hypoplasia. In the pharmacology of hypertension management, clinicians must always confirm a negative pregnancy test before initiating RAAS inhibitors.
How do thiazide diuretics differ from loop diuretics in hypertension management?
Thiazide diuretics, like chlorthalidone, are the primary choice for essential hypertension because they have a longer duration of action and work in the distal convoluted tubule. Loop diuretics, such as furosemide, are typically reserved for patients with a reduced GFR or symptomatic heart failure. While loop diuretics are more potent for rapid fluid removal, they don’t provide the same sustained blood pressure reduction required for chronic hypertension management.
What is the “ACE cough” and what causes it pharmacologically?
The “ACE cough” is a dry, non-productive cough that affects approximately 5% to 20% of patients taking ACE inhibitors. It’s caused by the accumulation of bradykinin and substance P in the upper airways. Since ACE is responsible for breaking down these inflammatory mediators, inhibiting the enzyme leads to their buildup, which sensitizes the cough reflex. If the cough becomes intolerable, patients are usually switched to an ARB, which doesn’t affect bradykinin levels.
Which antihypertensive drugs are preferred for patients with chronic kidney disease (CKD)?
ACE inhibitors and ARBs are the preferred agents for patients with CKD, particularly those with albuminuria. These medications lower efferent arteriolar resistance, which reduces the mechanical strain on the glomerulus and slows the decline of renal function. However, clinicians must carefully monitor serum potassium and creatinine levels shortly after starting therapy, as these drugs can potentially cause hyperkalemia or an acute, but often transient, rise in creatinine.
Can beta-blockers be used as first-line therapy for essential hypertension?
Beta-blockers aren’t typically used as first-line therapy for uncomplicated essential hypertension in the latest 2025 ACC/AHA guidelines. While they effectively lower heart rate, they don’t reduce the risk of stroke as effectively as the “Big Four” classes. They’re primarily indicated when a patient has a compelling reason, such as a recent myocardial infarction, stable ischemic heart disease, or heart failure with reduced ejection fraction. Without these comorbidities, they remain second-line options.
What are the signs of hypertensive emergency vs. hypertensive urgency?
The primary distinction between hypertensive emergency and urgency is the presence of acute end-organ damage. A hypertensive emergency occurs when blood pressure exceeds 180/120 mmHg and is accompanied by acute damage to the brain, heart, or kidneys, such as a stroke or acute pulmonary edema. Hypertensive urgency involves the same elevated pressures but without immediate organ injury. Emergencies require intravenous medications in an ICU setting, while urgencies are often managed with oral agents.
How does Spironolactone help in resistant hypertension?
Spironolactone serves as a powerful fourth-line agent by acting as a competitive aldosterone antagonist. In the pharmacology of hypertension management, it’s particularly effective for resistant cases where the patient may have subclinical primary aldosteronism or excessive sodium retention. By blocking the mineralocorticoid receptor, it promotes sodium excretion and potassium retention, helping to reach blood pressure goals when standard combinations of ACE inhibitors, CCBs, and thiazides have failed.