Endocrine Pharmacology Study Guide: High-Yield Review for Boards and Clinical Practice
Can you confidently differentiate between the March 2026 approval of once-weekly Awiqli and the April 2026 biosimilar launch of Langlara while under the pressure of a board exam clock? It’s a common frustration to feel buried under an endless web of feedback loops and look-alike hormone names. Most clinicians and students struggle to keep the various insulin types straight, especially as new oral GLP-1 agonists like Foundayo continue to reshape the therapeutic landscape. This endocrine pharmacology study guide provides a high-yield framework to master these complexities and understand the physiological “why” behind every clinical application.
We’ve structured this review to help you pass your board exams and excel in clinical practice by integrating the latest 2026 AACE management algorithms. You’ll learn to quickly differentiate between drug classes and understand how Medicare’s new negotiated prices for 2026 impact patient access to medications like Januvia and Jardiance. By the end of this guide, you’ll have a clear, logical map of endocrine therapy that turns stressful memorization into genuine clinical mastery.
Key Takeaways
- Understand how the negative feedback loop serves as the central target for pharmacological intervention to simplify complex hormonal interactions.
- Differentiate between thyroid replacements and glucocorticoid potencies by focusing on half-lives and the specific zones of the adrenal cortex.
- Use this endocrine pharmacology study guide to master the mechanisms of insulin release and the critical differences between Type 1 and Type 2 diabetes management.
- Develop a high-yield study strategy that prioritizes prototype agents and drug classes to ensure success on board exams and in clinical practice.
The Endocrine Framework: Physiology Meets Pharmacology
The endocrine system functions as a complex network of ductless glands that release chemical messengers, known as hormones, directly into the circulatory system. These messengers travel to distant target tissues to regulate everything from metabolic rate to electrolyte balance. When you approach an endocrine pharmacology study guide, it’s vital to view these drugs not as isolated chemicals, but as tools to manipulate a finely tuned physiological equilibrium. Most pharmacological interventions aim to restore homeostasis by exploiting the body’s natural negative feedback loops. If the system detects a surplus of a specific hormone, it naturally inhibits further production; drugs often mimic or block this signal to achieve a therapeutic effect.
Clinicians typically categorize endocrine medications into three functional groups. Hormone replacement therapy supplements a deficiency, such as using Levothyroxine for hypothyroidism. Hormone antagonists, like methimazole, inhibit overactive glands. Finally, diagnostic agents, such as cosyntropin, help providers identify the source of a hormonal imbalance. For board exams and clinical practice, you’ll find that the vast majority of high-yield questions focus on the “Big Three” topics: thyroid regulation, diabetes management, and adrenal steroid therapy.
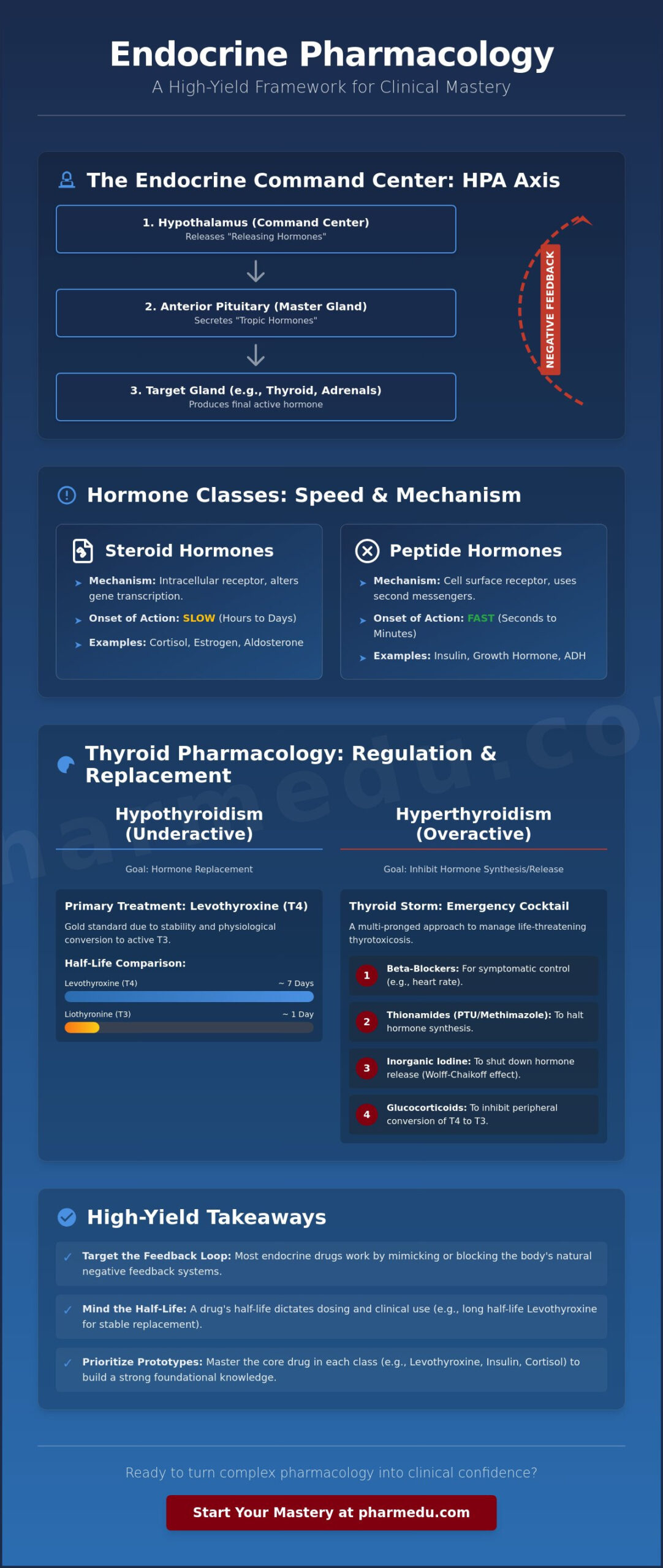
The Hypothalamic-Pituitary-Target Gland Axis
Understanding the hierarchy of the Endocrinology system is the first step in mastering this subject. The hypothalamus acts as the command center, releasing “releasing hormones” that stimulate the anterior pituitary. The pituitary then secretes “tropic hormones” that signal peripheral glands, like the thyroid or adrenal cortex, to produce the final active hormone. This hierarchy is essential for diagnosing disorders. A primary endocrine disorder involves a failure at the level of the target gland itself, while a secondary disorder stems from a pituitary malfunction. You’ll also need to account for the posterior pituitary, which stores and releases Vasopressin (ADH) and Oxytocin, both of which are critical in acute clinical settings.
Hormone Classes and Receptor Mechanisms
The chemical structure of a hormone dictates how it interacts with its target cell and how quickly you’ll see a clinical response. Steroid hormones, like cortisol and estrogen, are lipophilic and cross the cell membrane to bind with intracellular receptors. This process involves altering gene transcription, meaning the onset of action often takes hours or even days. In contrast, peptide hormones, such as insulin or growth hormone, bind to surface receptors and utilize second messenger systems. These drugs work rapidly, often within seconds or minutes. Hormone-receptor affinity dictates the concentration required to elicit a specific biological response, which directly determines the drug’s clinical potency.
Mastering this framework ensures you don’t just memorize drug names but understand the underlying logic of the system. This structural approach makes it much easier to predict side effects and therapeutic outcomes throughout your endocrine pharmacology study guide review.
Thyroid Pharmacology: Regulation and Replacement
Thyroid function begins with the active transport of iodide into follicular cells, where thyroid peroxidase (TPO) facilitates the synthesis of T3 and T4. While T3 is the more potent, active molecule, T4 serves as the primary reservoir. In any endocrine pharmacology study guide, the distinction between Levothyroxine (T4) and Liothyronine (T3) is a foundational concept. Levothyroxine remains the gold standard for replacement therapy due to its long half-life of approximately seven days, which allows for stable, once-daily dosing. Liothyronine, with its much shorter half-life and risk of peaks causing palpitations, is typically reserved for short-term use or specific diagnostic scenarios.
Managing an overactive thyroid requires thionamides: Methimazole and Propylthiouracil (PTU). Both drugs inhibit TPO, but PTU offers the additional benefit of blocking the peripheral conversion of T4 to T3. This makes PTU a critical component in treating “Thyroid Storm,” a life-threatening thyrotoxicosis. The emergency cocktail for this condition includes beta-blockers for symptomatic control, thionamides to halt synthesis, inorganic iodine to shut down hormone release via the Wolff-Chaikoff effect, and glucocorticoids to further inhibit peripheral conversion. Using a structured endocrine pharmacology study guide helps you organize these complex emergency protocols into a clear clinical timeline.
Hypothyroidism and Levothyroxine Management
Levothyroxine is the preferred replacement because the body naturally converts it into the active T3 form as needed, maintaining a physiological balance that T3-only supplements can’t match. Counseling patients on administration is vital for treatment success. The medication must be taken on an empty stomach, at least 30 to 60 minutes before breakfast. Absorption is significantly impaired by common supplements like calcium or iron; patients should separate these by at least four hours. Clinicians monitor success via TSH levels, but because of the drug’s long half-life, it takes roughly six to eight weeks to reach a new steady state after a dose adjustment. For a more interactive way to test your knowledge on these specific drug interactions, you can review our pharmacology practice quizzes designed for clinical mastery.
Hyperthyroidism: PTU vs. Methimazole
Pregnancy presents a unique pharmacological challenge in hyperthyroidism management. PTU is the drug of choice during the first trimester to avoid methimazole-associated birth defects. However, clinicians often switch patients to Methimazole for the remainder of the pregnancy to mitigate the higher risk of severe hepatotoxicity associated with PTU. Regardless of the agent, you must monitor for agranulocytosis. If a patient on thionamides develops a sudden fever or sore throat, they need an immediate white blood cell count check to rule out this rare but life-threatening side effect.
Diabetes Mellitus: Insulin and Oral Hypoglycemics
Diabetes management is a cornerstone of any endocrine pharmacology study guide, requiring a deep understanding of both absolute and relative insulin deficiencies. Type 1 Diabetes Mellitus involves the autoimmune destruction of pancreatic beta cells, leading to an absolute lack of insulin. In contrast, Type 2 Diabetes is characterized by peripheral insulin resistance and a progressive decline in beta cell function. To understand how we treat these conditions, we must first look at how the body naturally releases insulin. Glucose enters the beta cell via GLUT2 transporters, leading to increased ATP production. This rise in ATP closes the ATP-sensitive K+ channels, causing cell depolarization and an influx of calcium, which ultimately triggers the exocytosis of insulin granules.
When physiology fails, pharmacological intervention becomes necessary. The goal is often to mimic the natural meal-time spikes and baseline insulin levels through a basal-bolus regimen. If a patient’s blood glucose drops dangerously low, typically below 70 mg/dL, hypoglycemia management becomes the priority. While conscious patients can ingest simple carbohydrates, unconscious patients require an injection of glucagon. Glucagon works by stimulating hepatic glycogenolysis and gluconeogenesis, rapidly raising blood glucose levels to prevent neurological damage.
Insulin Pharmacokinetics: Rapid to Ultra-Long Acting
Clinicians use different insulin analogs by modifying the amino acid sequence of the human insulin molecule to alter its absorption and duration. For example, rapid-acting analogs like Lispro prevent the formation of hexamers, allowing for immediate dissociation into monomers and faster entry into the bloodstream.
- Lispro/Aspart (Rapid): Onset < 15 min; Peak 1 hour; Duration 3-5 hours.
- Regular (Short): Onset 30-60 min; Peak 2-3 hours; Duration 5-8 hours.
- NPH (Intermediate): Onset 2-4 hours; Peak 4-10 hours; Duration 10-16 hours.
- Glargine (Ultra-Long): Onset 1-2 hours; Peakless; Duration 24+ hours.
Insulin glargine achieves a peakless profile because it is formulated at an acidic pH of 4.0, which causes it to precipitate into microcrystals upon injection into the neutral pH of subcutaneous tissue, resulting in a slow and steady release into the systemic circulation.
Non-Insulin Injectables and Oral Agents
Metformin remains the first-line therapy for most Type 2 patients because it activates AMP-activated protein kinase (AMPK), which reduces hepatic gluconeogenesis and improves peripheral glucose uptake. While highly effective, it’s often associated with gastrointestinal distress and long-term vitamin B12 deficiency. Clinicians must also be vigilant about the risk of lactic acidosis in patients with significant renal impairment.
Modern therapy has expanded to include SGLT2 inhibitors, or “flozins,” which block glucose reabsorption in the proximal convoluted tubule. Beyond glycemic control, these agents offer significant cardiovascular and renal protection, particularly in patients with heart failure. GLP-1 receptor agonists, the “tides,” mimic the incretin effect, stimulating insulin secretion only when glucose levels are elevated. This glucose-dependent mechanism provides excellent weight loss benefits with a very low risk of hypoglycemia. Mastering these distinctions is a vital part of using an endocrine pharmacology study guide to prepare for real-world clinical decision-making.
Adrenal Steroids and Calcium Homeostasis
The adrenal cortex is organized into three distinct layers, each responsible for producing specific steroid hormones. A common mnemonic to remember these is “Salt, Sugar, Sex,” which corresponds to the zones from superficial to deep. The zona glomerulosa produces mineralocorticoids like aldosterone to regulate salt balance. The zona fasciculata synthesizes glucocorticoids, primarily cortisol, to manage glucose metabolism. Finally, the zona reticularis produces androgens. Mastering these anatomical and functional divisions is a core requirement for any endocrine pharmacology study guide aimed at clinical or board preparation.
Glucocorticoids are classified based on their anti-inflammatory potency and duration of action. Hydrocortisone is a short-acting agent that possesses significant mineralocorticoid activity, making it suitable for replacement therapy in adrenal insufficiency. Dexamethasone, however, is a long-acting, highly potent glucocorticoid with negligible mineralocorticoid effects. This makes it a preferred choice for treating conditions like cerebral edema where fluid retention must be avoided. To solidify your understanding of these steroid profiles, you can utilize our Interactive Pharmacology Flashcards to drill the specific potencies and clinical indications of each agent.
Glucocorticoids: Therapeutic Uses and Toxicities
Glucocorticoids achieve their anti-inflammatory effects by binding to intracellular receptors and modulating gene transcription. This process inhibits the synthesis of pro-inflammatory cytokines and enzymes like phospholipase A2. While effective, chronic use leads to a predictable cluster of “Cushingoid” side effects. Patients often experience hyperglycemia, osteoporosis, and a characteristic redistribution of fat to the trunk and face. They also suffer from thin skin and impaired wound healing. One of the most vital clinical rules involves HPA axis suppression. Exogenous steroids provide negative feedback that causes adrenal atrophy over time. If a patient stops therapy abruptly, they can’t produce enough endogenous cortisol to survive physiological stress, leading to a life-threatening adrenal crisis. Tapering doses is mandatory for any patient on long-term therapy.
Bone Mineral Metabolism and Pharmacotherapy
Calcium homeostasis is regulated by the interplay between Parathyroid Hormone (PTH), Vitamin D, and Calcitonin. Pharmacological management of bone loss focuses on either inhibiting resorption or stimulating formation. Bisphosphonates, the first-line treatment for osteoporosis, bind to hydroxyapatite and inhibit osteoclast activity. Because these drugs are poorly absorbed and highly irritating to the esophagus, patients must take them with a full glass of water and remain upright for at least 30 minutes.
In cases of chronic kidney disease, the body can’t convert Vitamin D into its active form. Providers must use Calcitriol, the active analog, to maintain calcium levels. For patients with high fracture risk, we choose between Teriparatide and Denosumab. Teriparatide is a recombinant PTH analog that acts as an anabolic agent when administered in daily pulses. Denosumab, conversely, is a monoclonal antibody that targets RANKL to provide potent antiresorptive effects. This endocrine pharmacology study guide helps you categorize these treatments so you can make informed decisions in a clinical setting.
Strategic Study Plan: Mastering Endocrine Pharmacology for Boards
Mastering this subject requires more than just staring at lists of hormones or memorizing names by rote. A truly effective endocrine pharmacology study guide transforms passive reading into active clinical reasoning. You should start by mastering the underlying feedback loops. If you don’t understand how the pituitary responds to low cortisol, you won’t understand why we taper steroids or how we diagnose adrenal insufficiency. Once the physiology is clear, group drugs by their class and focus on the “prototype” agent. If you know the side effects and mechanism of Metformin, you’ve already mastered the primary concerns for the entire biguanide class.
The third step involves shifting from theory to clinical context. Boards don’t just ask for a drug’s mechanism; they ask which drug is safest for a pregnant patient with a thyroid storm or how to adjust insulin for a patient who is fasting. Finally, you must implement active recall. Use flashcards and practice quizzes to test your memory on contraindications and monitoring parameters until the information becomes second nature. This systematic approach ensures you aren’t just memorizing facts, but building a framework for safe clinical practice.
Why High-Yield Video Vignettes Beat Textbooks
Traditional textbooks often fail to capture the dynamic nature of hormonal regulation. PharmEDU’s video vignettes bridge the gap between abstract theory and the high-pressure environment of an exam. These videos utilize visual storytelling to illustrate complex pathways like the HPA axis or the RAAS, making them far easier to retain than static diagrams. This micro-learning approach is specifically designed for busy healthcare students who need to maximize their study efficiency in short bursts. Visualizing the “why” behind a drug’s action helps you predict side effects rather than memorizing them from a list.
Integrating Case Studies into Your Review
Applying your knowledge to a patient scenario is the ultimate test of mastery. Clinical cases force you to weigh competing priorities, such as selecting a diabetes medication for a patient who also has heart failure. In these situations, the cardiovascular benefits of SGLT2 inhibitors discussed in previous sections become a decisive factor. Transitioning to comprehensive pharmacy review platforms allows you to interact with these scenarios in a way that static guides cannot match. These digital tools adapt to your performance, highlighting areas where your understanding of monitoring or contraindications might be weak.
To ensure you’re fully prepared for clinical practice or your next board exam, use this final checklist for every drug class in your endocrine pharmacology study guide review:
- Mechanism of Action (MOA): How does the drug interact with the receptor or feedback loop?
- Side Effects: What are the most common and most life-threatening adverse reactions?
- Contraindications: When is this drug absolutely prohibited, such as in pregnancy or renal failure?
- Monitoring: Which labs, like TSH, A1c, or electrolytes, are required to ensure safety and efficacy?
Elevate Your Clinical Mastery in Endocrine Pharmacology
Mastering the endocrine system requires you to move beyond simple memorization and embrace the physiological logic of feedback loops. By understanding how drugs like glucocorticoids or thionamides interact with the hypothalamic-pituitary axis, you can predict clinical outcomes and avoid dangerous complications like adrenal crisis. This endocrine pharmacology study guide has outlined the high-yield frameworks necessary for board success, from the peakless profile of insulin glargine to the critical timing of thyroid replacement. Precision in these details is what separates a student from a truly competent clinician.
Transitioning from theory to practice is easier when you have the right tools. Start your high-yield pharmacology review with PharmEDU today! Our platform, designed by healthcare educators, offers 100+ high-yield video vignettes, interactive flashcards, and practice quizzes to solidify your knowledge. You don’t have to face the pressure of boards alone. With a structured approach and active recall, you’ll gain the confidence to excel in both your exams and your future clinical practice.
Frequently Asked Questions
What is the most important feedback loop to know for endocrine pharmacology?
The Hypothalamic-Pituitary-Target Gland axis is the most critical feedback loop for mastering this subject. It controls the majority of peripheral hormonal functions, including thyroid and adrenal activity. When you understand how the hypothalamus senses low hormone levels to release tropic signals, you can accurately interpret diagnostic labs. This knowledge is essential for identifying whether a disorder is primary or secondary in origin.
How do I remember the difference between PTU and Methimazole for hyperthyroidism?
You can remember the difference by focusing on pregnancy trimesters and peripheral action. PTU is the preferred agent during the first trimester, while Methimazole is used for the remainder of the pregnancy. Additionally, PTU is unique because it inhibits the peripheral conversion of T4 to T3. This specific mechanism is why it remains a staple in treating acute, life-threatening thyroid storm.
Why is Metformin the first-line treatment for Type 2 Diabetes?
Metformin is the first-line choice because it effectively lowers A1c without causing weight gain or significant hypoglycemia. It works primarily by activating AMPK to suppress hepatic glucose production and improve insulin sensitivity. Because it doesn’t stimulate insulin secretion from the pancreas, it carries a much lower risk of dangerous blood sugar drops compared to other oral agents like sulfonylureas.
What are the common side effects of long-term corticosteroid use?
Chronic corticosteroid use leads to a cluster of metabolic and physical changes known as Cushingoid features. Patients often develop hyperglycemia, osteoporosis, and a characteristic redistribution of body fat to the trunk and neck. You’ll also see skin thinning and delayed wound healing. These side effects occur because steroids influence gene transcription across almost every tissue in the body over time.
Can I use this study guide for the NAPLEX or NCLEX exams?
This endocrine pharmacology study guide is specifically designed to align with the high-yield topics found on the NAPLEX and NCLEX exams. It prioritizes the clinical counseling points and safety monitoring that these licensing boards emphasize. Whether you’re a pharmacy or nursing student, mastering these drug classes and their prototype agents is a critical step toward passing your professional boards.
What is the difference between primary and secondary adrenal insufficiency?
Primary adrenal insufficiency occurs when the adrenal gland itself is damaged, while secondary insufficiency stems from a pituitary failure. In primary disease, you’ll see high ACTH levels as the body tries to stimulate the non-functional gland. In secondary disease, ACTH levels are low or inappropriately normal because the pituitary isn’t sending the necessary signal to the adrenal cortex to produce cortisol.
How do SGLT2 inhibitors help patients with heart failure?
SGLT2 inhibitors benefit heart failure patients by promoting natriuresis and osmotic diuresis to reduce fluid overload. By blocking glucose reabsorption in the proximal tubule, they lower blood pressure and decrease the workload on the heart. These drugs also improve cardiac energy metabolism and reduce the risk of hospitalization for patients with both reduced and preserved ejection fractions in clinical settings.
Why must Levothyroxine be taken on an empty stomach?
Levothyroxine requires an acidic gastric environment for proper absorption into the bloodstream. Taking it with food, or with supplements like calcium and iron, can significantly decrease its bioavailability and lead to inconsistent TSH levels. Patients should take this medication at least 30 to 60 minutes before breakfast with a full glass of water to ensure stable and predictable therapeutic results.