Lipid-Lowering Drugs Study Guide: High-Yield Pharmacology for 2026
What if the secret to mastering lipid pharmacology isn’t endless rote memorization, but simply mapping the metabolic pathways of the liver? It’s a common frustration to feel buried under a mountain of drug names while trying to distinguish the clinical nuances of fibrates from statins or deciding when to escalate to non-statin therapies. This lipid-lowering drugs study guide is designed to alleviate that burden by providing a high-yield framework for the 2026 ACC/AHA guidelines, ensuring you stay ahead of the curve in a field where 1 in 4 U.S. adults now faces high LDL-C levels.
We’ll bridge the gap between complex biochemistry and clinical practice, helping you understand the “why” behind the new PREVENT-ASCVD risk calculator and the latest LDL-C treatment goals, such as the sub-55 mg/dL target for very high-risk patients. By focusing on the mechanisms that drive these therapies, you’ll gain the confidence to apply lipid pharmacology to real-world case studies and excel on your board exams. This guide simplifies the transition toward more aggressive, personalized intervention strategies currently defining the standard of care.
We’ll explore everything from the foundational role of statins to the clinical arrival of third-generation PCSK9 inhibitors like Lerochol. This review breaks down critical drug-drug interactions and provides the clarity you need to manage patient care with professional authority and scientific rigor.
Key Takeaways
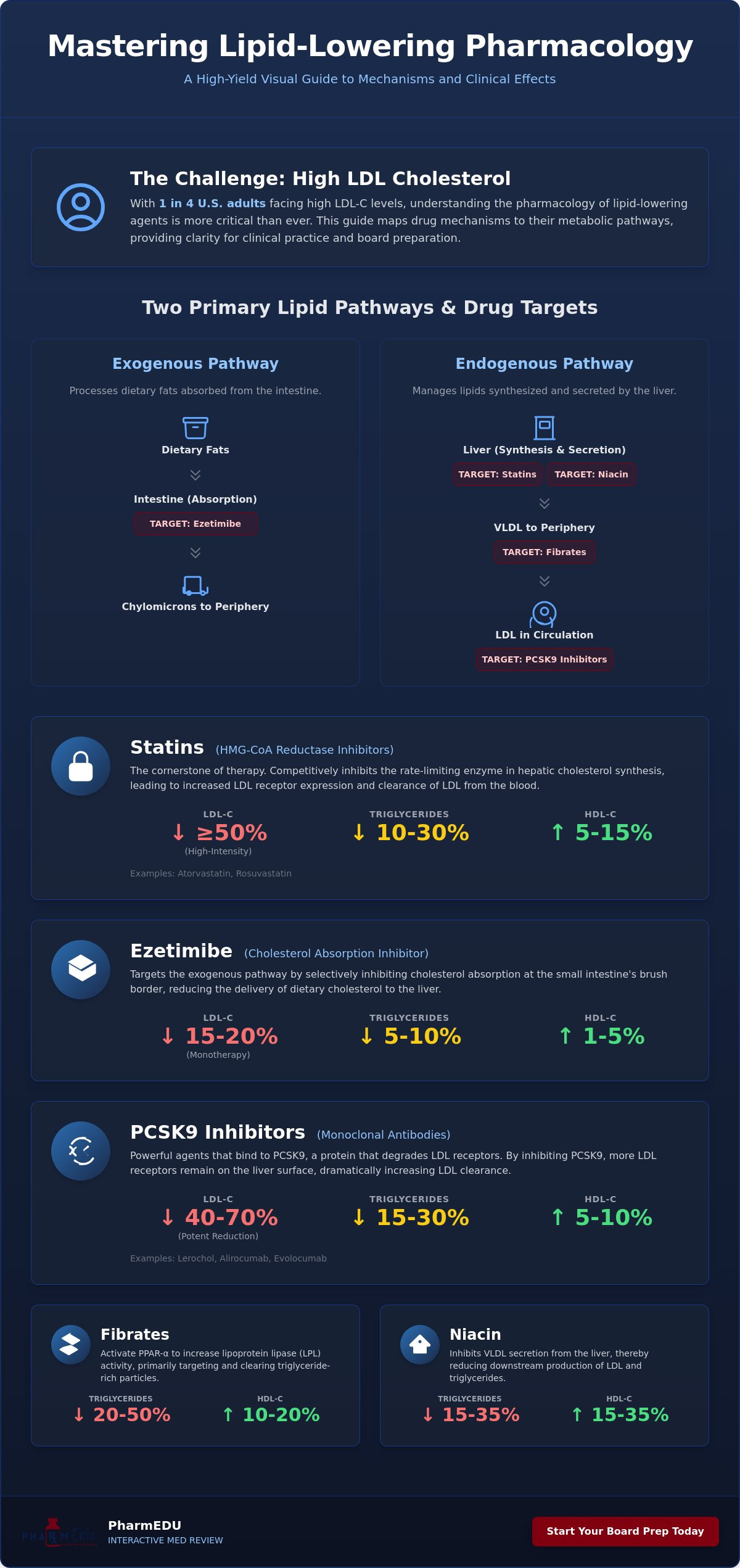
- Master the distinction between exogenous and endogenous lipid pathways to understand how specific agents target dietary absorption versus hepatic synthesis.
- Utilize this lipid-lowering drugs study guide to differentiate between high-intensity and moderate-intensity statin regimens based on competitive HMG-CoA reductase inhibition.
- Explore the unique mechanisms of non-statin therapies, including the brush-border action of Ezetimibe and the monoclonal antibody delivery of PCSK9 inhibitors.
- Identify the clinical roles of fibrates and niacin in managing hypertriglyceridemia through PPAR-α activation and VLDL secretion inhibition.
- Streamline your board preparation by applying the latest 2026 risk assessment tools and determining the appropriate timing for lipid panels and monitoring parameters.
Fundamentals of Lipid Physiology and Lipoprotein Metabolism
Lipids are essential for life. They form the structural basis of cell membranes and provide the raw materials for steroid hormones. Triglycerides act as a vital energy reservoir. However, when the balance shifts, these same molecules drive the progression of atherosclerotic cardiovascular disease (ASCVD). Mastering this lipid-lowering drugs study guide requires looking past the names and focusing on the underlying physiology. If you understand how the liver manages these molecules, the pharmacology becomes intuitive.
The body manages lipids through two distinct routes. The exogenous pathway handles dietary fats, where chylomicrons transport lipids from the intestine to peripheral tissues. Conversely, the endogenous pathway begins in the liver, where VLDL is secreted to deliver hepatic lipids. A comprehensive overview of lipid-lowering agents reveals that most medications target specific intersections of these two pathways to restore homeostatic balance.
The Lipoprotein Transport System
Lipoproteins are classified by their density and protein content. Chylomicrons are the largest and least dense particles, carrying mostly triglycerides. As they lose these fats via Lipoprotein Lipase (LPL), they become remnants. In the endogenous track, VLDL transforms into Intermediate-Density Lipoprotein (IDL) and finally into Low-Density Lipoprotein (LDL). LDL is often labeled “bad” cholesterol because it delivers cholesterol to peripheral tissues, including the arterial walls. This transport system is the primary target for most interventions mentioned in this lipid-lowering drugs study guide.
Apolipoproteins act as the “GPS” for these particles. ApoB is found on all potentially atherogenic particles, including VLDL, IDL, and LDL. This makes it a critical marker of cardiovascular risk. In contrast, ApoA-I is the primary protein on High-Density Lipoprotein (HDL). HDL facilitates reverse cholesterol transport, a process that moves excess cholesterol from the tissues back to the liver for excretion. This protective role explains why HDL is considered “good” cholesterol in clinical settings.
Key Physiological Enzymes and Receptors
Three primary molecular players dictate how we treat dyslipidemia. HMG-CoA reductase is the rate-limiting enzyme in hepatic cholesterol synthesis. When we inhibit this enzyme, we don’t just stop production; we trigger a compensatory increase in LDL receptors. The LDL Receptor (LDLR) is the liver’s primary tool for cleaning the blood. It pulls LDL particles out of circulation and into the hepatocyte for processing.
Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) is a protein that regulates these receptors. It promotes the degradation of LDLR, which reduces the liver’s ability to clear LDL. By inhibiting PCSK9, we keep more receptors on the cell surface. Finally, Lipoprotein Lipase (LPL) serves as the gatekeeper for triglyceride clearance. It sits on the capillary walls of adipose and muscle tissue, breaking down triglycerides for energy use or storage. These enzymes aren’t just biological concepts; they’re the specific locks that our pharmacological “keys” are designed to open.
First-Line Therapy: HMG-CoA Reductase Inhibitors (Statins)
Statins remain the cornerstone of pharmacological management for dyslipidemia. Their primary mechanism involves the competitive inhibition of HMG-CoA reductase, the rate-limiting enzyme in the mevalonate pathway. By blocking this enzyme, statins reduce hepatic cholesterol synthesis. This intracellular depletion triggers a critical compensatory response: the up-regulation of LDL receptors on the hepatocyte surface. These increased receptors actively clear LDL particles from the systemic circulation, effectively lowering plasma levels. Any professional lipid-lowering drugs study guide must emphasize that the reduction in LDL-C is dose-dependent, though it follows the “rule of six,” where doubling the dose only yields an additional 6% reduction.
Clinical guidelines categorize statins by intensity. High-intensity regimens, such as Atorvastatin 40-80 mg or Rosuvastatin 20-40 mg, aim for a ≥50% reduction in LDL-C. Moderate-intensity doses target a 30% to 49% reduction. Beyond simple lipid lowering, statins provide pleiotropic benefits. They stabilize atherosclerotic plaques, improve endothelial function, and reduce systemic inflammation. These effects explain why statins often provide cardiovascular protection even before significant changes in lipid profiles occur. To reinforce these concepts during your prep, utilizing interactive pharmacology flashcards can help solidify the dosing and intensity categories required for board exams.
Safety monitoring focuses on liver transaminases and muscle toxicity. While a transient rise in LFTs is common, true hepatotoxicity is rare. Myopathy remains the most frequent concern, ranging from mild myalgia to life-threatening rhabdomyolysis. According to the Comprehensive Guide to Lipid-Lowering Drugs, clinicians should establish baseline CK levels only in high-risk patients, as routine monitoring isn’t typically indicated unless symptoms arise.
Pharmacokinetics and Drug Interactions
Metabolism varies significantly across the class. Atorvastatin, Lovastatin, and Simvastatin are metabolized by CYP3A4, making them prone to interactions with inhibitors like grapefruit juice, clarithromycin, or protease inhibitors. Rosuvastatin and Pitavastatin bypass this pathway, primarily using CYP2C9 or minimal metabolism, which offers a safer profile for polypharmacy patients. Lipophilic statins like Simvastatin cross cell membranes easily, whereas hydrophilic options like Pravastatin and Rosuvastatin may have a lower incidence of muscle-related side effects. Statins with short half-lives, such as Simvastatin, must be taken at night to coincide with the peak of endogenous cholesterol synthesis.
Managing Statin Intolerance
Distinguishing between Statin-Associated Muscle Symptoms (SAMS) and true rhabdomyolysis is vital for clinical decision-making. SAMS usually presents as bilateral, proximal muscle pain without significant CK elevation. If a patient reports intolerance, the first step is a “washout” period followed by a re-challenge with a different statin or an alternate-day dosing schedule. The Statin Ladder approach involves starting with the highest tolerated statin dose and then layering non-statin therapies like Ezetimibe or Bempedoic acid to reach the patient’s goal LDL-C. This structured escalation ensures that even those with sensitivities achieve necessary cardiovascular risk reduction.
Advanced LDL Reduction: PCSK9 Inhibitors and Ezetimibe
When statins alone don’t reach therapeutic targets, clinicians turn to advanced agents that target different metabolic intersections. This lipid-lowering drugs study guide highlights the shift toward combination therapy as the standard for high-risk patients. Ezetimibe remains the most common second-line addition, but the emergence of PCSK9-targeted therapies and ACLY inhibitors has transformed the management of refractory hypercholesterolemia. These agents are particularly vital for patients with Familial Hypercholesterolemia or those who’ve suffered a cardiovascular event despite being on a high-intensity statin regimen.
Ezetimibe and Bile Acid Sequestrants
Ezetimibe works at the intestinal brush border by selectively inhibiting the NPC1L1 protein. This action prevents the absorption of both dietary and biliary cholesterol. It’s particularly effective when paired with a statin because it creates a dual-blockade: the statin stops synthesis while Ezetimibe stops absorption. This synergy allows for significant LDL-C reduction without always needing to maximize statin doses, which can help mitigate side effects.
Bile acid sequestrants, such as Cholestyramine and Colesevelam, take a more mechanical approach. They bind bile acids in the gut and interrupt enterohepatic circulation. This forces the liver to convert its own cholesterol stores into new bile acids, which upregulates LDL receptors. While these are some of the oldest tools in the lipid-lowering drugs study guide, their use is often limited by practical constraints:
- Frequent gastrointestinal side effects like bloating and constipation.
- Interference with the absorption of fat-soluble vitamins (A, D, E, and K).
- Potential to increase triglyceride levels in patients with pre-existing hypertriglyceridemia.
The PCSK9 Revolution
The most significant advancement in LDL management involves the PCSK9 protein. Under normal conditions, PCSK9 binds to LDL receptors and marks them for lysosomal degradation. By inhibiting this protein with monoclonal antibodies (mAbs) like Alirocumab and Evolocumab, we allow receptors to recycle back to the cell surface multiple times. This leads to a dramatic drop in systemic LDL levels, often by 50% to 60%. For clinicians managing complex cases, resources like Lipid-Lowering Therapy for Clinicians provide detailed protocols for these injectable therapies.
Newer options are further refining this approach. Inclisiran uses small interfering RNA (siRNA) to stop the liver from producing PCSK9 in the first place. Instead of bi-weekly injections required for mAbs, patients receive Inclisiran just twice a year, which significantly improves long-term adherence. For those who can’t tolerate statins due to muscle symptoms, Bempedoic acid offers a unique solution. It inhibits adenosine triphosphate-citrate lyase (ACLY), an enzyme upstream of HMG-CoA reductase. Because it’s a prodrug that requires activation by an enzyme found only in the liver, it avoids muscle tissue entirely, reducing the risk of myalgia.
Targeting Triglycerides: Fibrates, Niacin, and Omega-3s
While previous sections of this lipid-lowering drugs study guide focused on LDL-C reduction, managing elevated triglycerides (TGs) is equally critical for patient safety. Severe hypertriglyceridemia, defined as levels above 500 mg/dL, significantly increases the risk of acute pancreatitis. In these scenarios, the clinical priority shifts from long-term cardiovascular risk to immediate metabolic stabilization. Fibrates, niacin, and high-dose omega-3 fatty acids are the primary agents used to address these specific lipid abnormalities.
Fibrates and PPAR-alpha Activation
Fibrates, such as Gemfibrozil and Fenofibrate, are the most potent TG-lowering agents available. They function as agonists for the peroxisome proliferator-activated receptor-alpha (PPAR-α), a nuclear receptor that regulates lipid metabolism. Activation of PPAR-α leads to the upregulation of Lipoprotein Lipase (LPL), which accelerates the clearance of triglyceride-rich lipoproteins. It also increases fatty acid oxidation in the liver, further reducing VLDL production. To test your knowledge on these specific pathways, you can use our Pharmacology Practice Quizzes to ensure you’re ready for clinical rotations.
Clinicians must be cautious when combining fibrates with statins. Gemfibrozil is particularly problematic because it inhibits the glucuronidation of statins and competes for the OATP1B1 transporter. This interaction significantly raises statin plasma concentrations, increasing the risk of rhabdomyolysis. Fenofibrate is generally preferred in combination therapy as it doesn’t share this same metabolic interference. Additionally, Fenofibrate requires careful renal dosing, as it’s primarily excreted by the kidneys and can cause a transient, though usually benign, rise in serum creatinine.
Niacin: The High-Yield Side Effect Profile
Niacin, or Vitamin B3, lowers lipids by inhibiting the lipolysis of triglycerides in adipose tissue and reducing VLDL secretion from the liver. While it effectively raises HDL-C, its clinical use has waned due to a challenging side-effect profile. The most notorious reaction is cutaneous flushing, mediated by the release of Prostaglandin D2. Patients can mitigate this by taking 325 mg of Aspirin 30 minutes before their niacin dose and avoiding hot liquids or spicy foods, which can exacerbate vasodilation.
Metabolic concerns also limit niacin’s utility. It can decrease insulin sensitivity, leading to hyperglycemia in diabetic patients, and compete with uric acid for excretion, potentially triggering gout flares. Despite these drawbacks, niacin remains a high-yield topic for board exams due to its unique mechanism and predictable adverse effects. Omega-3 fatty acids, particularly icosapent ethyl, provide a safer alternative for TG reduction. They work by inhibiting hepatic VLDL synthesis and enhancing TG clearance, often without the metabolic baggage associated with niacin therapy.
Clinical Application and Board Exam Preparation Strategies
Translating pharmacological theory into clinical success requires a structured approach to risk assessment. The 2026 guidelines emphasize the use of the PREVENT-ASCVD risk calculator to estimate 10 and 30 year cardiovascular risk for adults aged 30 to 79. This tool replaces the older Pooled Cohort Equations and provides a more nuanced view for primary prevention. When using this lipid-lowering drugs study guide for clinical rotations, remember that treatment isn’t just about the numbers; it’s about the patient’s total risk profile, including selective Coronary Artery Calcium (CAC) scoring for those in the intermediate risk category.
Monitoring parameters are a frequent source of confusion on exams. Clinicians should obtain baseline Liver Function Tests (LFTs) before starting statin therapy, but routine periodic monitoring is no longer recommended unless the patient develops symptoms of hepatotoxicity. In contrast, a follow-up lipid panel is typically ordered 4 to 12 weeks after starting or adjusting therapy to assess adherence and efficacy. Understanding these distinctions helps you avoid common “distractor” answers that suggest unnecessary lab work.
Contraindications remain high-yield territory. Statins are generally avoided during pregnancy due to their interference with essential cholesterol synthesis in the developing fetus. Patients with active liver disease should avoid most systemic lipid-lowering agents, while those with severe renal impairment require careful dose adjustments, particularly with Fenofibrate. To keep these safety profiles organized, many students find that a lipid-lowering drugs study guide centered on active recall is the most efficient way to prepare.
Board-Style Case Study Analysis
Exam questions often present a patient with multiple comorbidities, such as Diabetes Mellitus and established Coronary Artery Disease. In these scenarios, the answer is almost always high-intensity statin therapy, regardless of the baseline LDL-C, because the patient is already at very high risk. Watch out for “red herrings” like minor, non-specific muscle aches that don’t meet the criteria for Statin-Associated Muscle Symptoms (SAMS). For a deeper look at how digital tools are replacing traditional methods for these complex cases, see our Comprehensive Pharmacy Review.
Study Resources and Memory Tools
Mastering this volume of information requires more than passive reading. Utilizing Pharmacology Flashcards allows you to drill mechanism-specific details, such as the NPC1L1 target for Ezetimibe versus the PPAR-α target for fibrates. Visual learners often benefit from High-Yield Video Vignettes that illustrate the recycling of LDL receptors. As you approach your final review, consult our NAPLEX Prep Course checklist to ensure no high-yield topic, from the new 2026 LDL goals to the latest PCSK9 inhibitors, is left to chance.
Advancing Your Clinical Expertise in Lipid Management
Success in modern cardiovascular care requires more than just knowing drug names; it demands a deep understanding of metabolic pathways and the latest 2026 clinical guidelines. We’ve explored how statins remain the first line of defense and why the integration of non-statin therapies like PCSK9 inhibitors is now essential for high-risk patients. By mastering the nuances of this lipid-lowering drugs study guide, you’re better prepared to navigate complex risk assessments and provide evidence-based care that meets today’s aggressive LDL-C targets.
Transitioning from a student to a confident practitioner is a journey of continuous learning. To streamline your preparation, you can Master Pharmacology with PharmEDU’s High-Yield Study Platform. Our resources cover over 100 high-yield topics through mobile-compliant micro-learning segments designed for busy professionals. You’ll gain access to expert-led video vignettes and interactive quizzes that turn abstract mechanisms into practical knowledge. Stay committed to your professional development, and you’ll find that even the most complex pharmacological challenges become manageable with the right partners by your side.
Frequently Asked Questions
What is the most effective drug class for lowering LDL cholesterol?
PCSK9 inhibitors, such as Evolocumab and Alirocumab, are currently the most effective drug class for lowering LDL cholesterol, often achieving reductions of 50% to 60%. While statins remain the first-line choice for most patients, these injectables provide superior reduction for those with refractory hypercholesterolemia or familial conditions. They work by increasing the density of LDL receptors on the liver’s surface, which allows for more efficient clearance of cholesterol particles from the bloodstream.
How do Statins actually work at the molecular level?
Statins work by competitively inhibiting HMG-CoA reductase, the rate-limiting enzyme in the hepatic mevalonate pathway. This inhibition stops the liver from synthesizing its own cholesterol, leading to a drop in intracellular levels. The liver responds by upregulating LDL receptors on the cell surface to pull cholesterol from the systemic circulation. This dual action of blocking synthesis and increasing clearance is a fundamental concept in any lipid-lowering drugs study guide.
Why is it dangerous to combine Gemfibrozil with certain Statins?
Combining Gemfibrozil with statins is dangerous because it significantly increases the risk of myopathy and life-threatening rhabdomyolysis. Gemfibrozil inhibits the specific glucuronidation pathway that most statins require for metabolism, which leads to toxic elevations in drug plasma concentrations. It also competes for the OATP1B1 hepatic uptake transporter. If a patient requires both a statin and a fibrate, Fenofibrate is the preferred clinical choice because it doesn’t interfere with statin metabolism in this way.
What are the common side effects of Niacin and how can they be managed?
Cutaneous flushing, itching, and a sensation of warmth are the most common side effects of Niacin, triggered by the release of prostaglandin D2. Patients can manage these symptoms by taking 325 mg of Aspirin approximately 30 minutes before their Niacin dose to block prostaglandin synthesis. It’s also helpful to take the medication with food and avoid hot beverages or spicy meals near the time of administration. Long-term use requires monitoring for metabolic changes like hyperglycemia and hyperuricemia.
When are PCSK9 inhibitors typically prescribed?
PCSK9 inhibitors are typically prescribed for high-risk patients with established cardiovascular disease or Familial Hypercholesterolemia who haven’t reached their LDL-C goals on maximally tolerated statins. They’re also a vital option for patients with documented statin intolerance. The 2026 guidelines emphasize their use when LDL-C remains above 55 mg/dL for very high-risk secondary prevention. These medications are administered via subcutaneous injection every two weeks or once monthly depending on the specific agent.
Can lipid-lowering drugs be used during pregnancy?
Most lipid-lowering drugs, particularly statins, are contraindicated during pregnancy because cholesterol is essential for fetal membrane synthesis and hormone production. Inhibiting these pathways can lead to serious developmental risks for the fetus. Bile acid sequestrants like Colesevelam are sometimes considered if treatment is absolutely necessary because they aren’t absorbed into the systemic circulation. However, the standard of care is generally to pause lipid therapy until the patient has finished pregnancy and breastfeeding.
What is the difference between Ezetimibe and Bile Acid Sequestrants?
Ezetimibe selectively inhibits the NPC1L1 transporter at the intestinal brush border to block the absorption of dietary cholesterol. In contrast, bile acid sequestrants like Cholestyramine bind bile acids in the gut and prevent their reabsorption, forcing the liver to convert its own cholesterol stores into new bile acids. While both target the exogenous pathway, Ezetimibe is generally better tolerated. Sequestrants often cause significant gastrointestinal distress and can interfere with the absorption of fat-soluble vitamins.
How often should liver enzymes be monitored when starting a Statin?
Liver enzymes should be measured at baseline before starting a statin, but routine periodic monitoring is no longer recommended for asymptomatic patients. Clinicians should only re-test transaminases if the patient develops clinical signs of hepatotoxicity, such as jaundice, dark urine, or unusual fatigue. This evidence-based approach is a key part of a modern lipid-lowering drugs study guide, as it reduces unnecessary testing while maintaining patient safety. Adherence to this protocol aligns with the latest professional standards for 2026.