Pharmacology of Anesthetics for Students: The High-Yield Study Guide
Why does the most “potent” anesthetic often take the longest to reach the brain? If the inverse relationship between blood-gas solubility and induction speed still feels like a mental hurdle, you’re certainly not alone. Most medical and pharmacy students feel overwhelmed by the sheer volume of agents, especially with recent developments like the June 2026 FDA approval of Cypsedo. It’s easy to get lost in the sea of MAC values and side effect profiles while trying to master the pharmacology of anesthetics for students.
We understand that you need more than just a list of drugs; you need a logical framework for the physiologic triad of amnesia, analgesia, and immobility. This high-yield review promises to clarify the complex mechanisms and kinetics of both general and local anesthetics. We’ll break down the blood-gas partition coefficient, explain why the MAC for Sevoflurane is 2.1% for a 40-year-old, and provide the board-focused precision required to answer clinical questions with absolute confidence.
Key Takeaways
- Understand the physiologic triad of amnesia, analgesia, and muscle relaxation to move beyond the simple concept of “sleep” in general anesthesia.
- Master the inverse relationship between the blood-gas partition coefficient and induction speed to accurately predict how quickly volatile gases take effect.
- Compare the clinical profiles of common induction agents to build a strong foundation in the pharmacology of anesthetics for students.
- Utilize the “Two-I” mnemonic to instantly distinguish between ester and amide local anesthetics during high-pressure exams.
- Learn to calculate the additive effects of nitrous oxide and volatile gases using the MAC concept for board-style scenarios.
Fundamentals of Anesthetic Pharmacology: The Triad of General Anesthesia
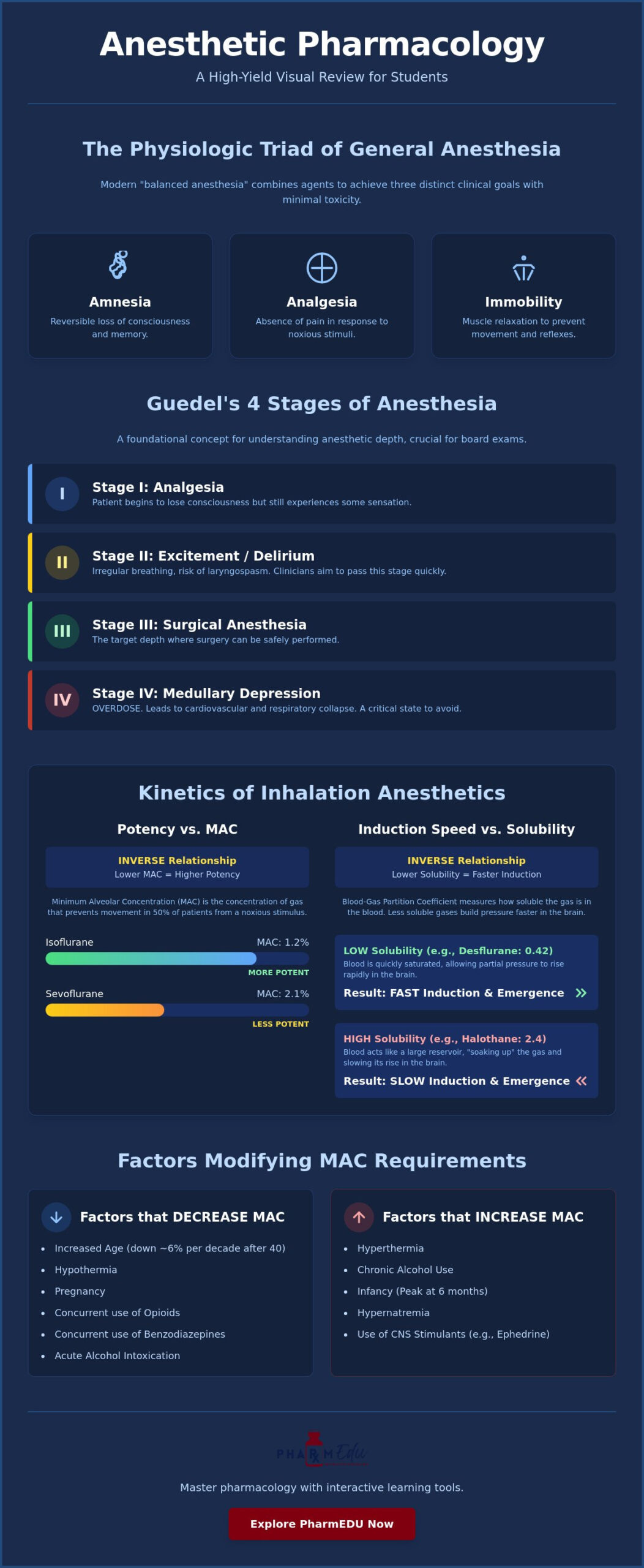
General anesthesia is often simplified as “putting a patient to sleep,” but for a clinician, it’s a precisely controlled, reversible state of central nervous system depression. This state ensures the patient remains safe and comfortable during invasive procedures. Understanding the pharmacology of anesthetics for students begins with mastering the “Anesthetic Triad.” This triad consists of three distinct clinical goals: amnesia (unconsciousness), analgesia (pain relief), and immobility (muscle relaxation). While some agents provide all three, most modern techniques utilize a “balanced anesthesia” approach, combining different drugs to achieve these goals with minimal toxicity.
Historically, Guedel’s stages provided a roadmap for monitoring anesthetic depth. While modern agents move through these phases rapidly, they remain essential for board exams:
- Stage I: Analgesia. The patient begins to lose consciousness but still feels some sensation.
- Stage II: Excitement. Characterized by irregular breathing and potential laryngospasm; clinicians aim to pass through this stage quickly.
- Stage III: Surgical Anesthesia. The target depth where surgery can safely proceed.
- Stage IV: Medullary Depression. An overdose state leading to cardiovascular and respiratory collapse.
Pharmacodynamics: How Anesthetics Alter Consciousness
Most general anesthetics work by enhancing inhibitory neurotransmission or inhibiting excitatory pathways. The primary target for most intravenous and volatile agents is the GABA-A receptor. By potentiating these receptors, drugs increase chloride conductance, which hyperpolarizes neurons and suppresses CNS activity. Ketamine is the notable exception, acting as an NMDA receptor antagonist to produce “dissociative anesthesia.” For years, the Meyer-Overton rule suggested that anesthetic potency was purely related to lipid solubility (Unitary Theory). However, modern research into General Anesthetic Pharmacology favors the Specific Receptor Theory, which identifies unique binding sites on protein receptors like GABA-A and two-pore domain potassium channels.
Pharmacokinetics in Anesthesia: The Concept of Context-Sensitive Half-Life
In the pharmacology of anesthetics for students, understanding drug movement is just as vital as knowing how they work. Standard elimination half-life is often misleading in anesthesia because it doesn’t account for drug redistribution. Highly lipid-soluble drugs like propofol quickly move from the blood into the brain for induction and then redistribute into muscle and fat, leading to emergence. This led to the development of a more practical metric for infusions. Context-sensitive half-life is the time required for plasma concentration to decrease by 50% after stopping an infusion. As the duration of an infusion increases, peripheral tissues become saturated, which can significantly prolong recovery times for certain agents.
Understanding these kinetics and the duration of drug effects is particularly important when managing patients during long-distance transfers. To see how clinical expertise is applied in these settings, you can explore Commercial Airline Medical Escort options provided by RN MEDflights for international patient support.
Inhalation Anesthetics: Potency, MAC, and Solubility
Understanding the pharmacology of anesthetics for students requires a firm grasp of the Minimum Alveolar Concentration (MAC). This value represents the concentration of a gas at one atmosphere that prevents skeletal muscle movement in 50% of patients responding to a noxious stimulus. Essentially, MAC is the standard measure of anesthetic potency. It’s important to remember that potency is inversely proportional to the MAC value. While Sevoflurane has a MAC of 2.1% for a 40-year-old adult, Isoflurane is significantly more potent with a MAC range of 1.15 to 1.28%.
Kinetics in inhalation anesthesia depend heavily on the blood-gas partition coefficient. This number describes the solubility of the gas in the blood compared to the alveolar air. A low coefficient, such as Desflurane’s 0.42, indicates the drug is poorly soluble. Because the blood doesn’t “soak up” the gas, the partial pressure in the alveoli rises rapidly, leading to faster induction and emergence. Conversely, more soluble agents take longer to reach equilibrium. If you’re finding these kinetic relationships difficult to visualize, our Interactive Pharmacology Flashcards provide a structured way to drill these essential coefficients.
Several physiological factors alter MAC requirements. For instance, MAC values decrease by approximately 6% per decade after the age of 40. Other factors that decrease MAC include hypothermia, pregnancy, and the concurrent use of opioids or benzodiazepines. Hyperthermia and chronic alcohol use typically increase the required concentration. Students must also master the “Second Gas Effect.” When a high concentration of Nitrous Oxide is administered alongside a volatile agent, the rapid uptake of Nitrous Oxide concentrates the remaining volatile gas in the alveoli, accelerating the induction of the second agent.
Differentiating Volatile Liquids: Isoflurane, Sevoflurane, and Desflurane
Sevoflurane is the clinical favorite for pediatric mask inductions. Its low pungency and non-irritating nature to the airway make it ideal for children who don’t yet have intravenous access. Desflurane offers the fastest emergence due to its extremely low solubility, though its high pungency can trigger coughing or laryngospasm. Isoflurane remains a staple for maintenance because it’s cost-effective and preserves cardiac output well, despite having a slower induction profile than its modern counterparts.
Nitrous Oxide: The Non-Volatile Exception
Nitrous Oxide is unique because it’s an inorganic gas with a MAC exceeding 100%, meaning it cannot produce surgical anesthesia alone at sea level. However, it provides excellent analgesia and is frequently used to reduce the MAC of more potent volatile gases. You must be cautious with its use in patients with closed gas spaces. Nitrous Oxide is 34 times more soluble in blood than Nitrogen. It can rapidly enter and expand gas-filled areas like a pneumothorax, the middle ear, or a bowel obstruction, potentially leading to dangerous pressure increases.
Intravenous Induction Agents: A Comparative Analysis
While inhalation agents are excellent for maintenance, intravenous (IV) agents provide the rapid, “arm-to-brain” circulation time required for a smooth induction. Mastering the pharmacology of anesthetics for students involves recognizing which agent fits a specific patient’s physiological needs. Propofol remains the current gold standard for induction. It works by potentiating GABA-A receptors, leading to nearly instantaneous unconsciousness. Beyond its role in induction, Propofol is highly valued for its antiemetic properties, which significantly reduces the risk of postoperative nausea and vomiting compared to volatile gases.
For the hemodynamically unstable patient, Etomidate is often the clinician’s first choice. It offers remarkable cardiovascular stability, making it ideal for patients with sepsis or heart failure. However, students must remember its primary clinical caveat: Etomidate causes transient adrenal suppression by inhibiting the enzyme 11-beta-hydroxylase. This effect can last for several hours after a single dose. Ketamine offers a different approach by providing “dissociative anesthesia” through NMDA receptor antagonism. Its role in modern behavioral health is also expanding; for more on clinical mental health assessments, you can explore Psychiatric Evaluation at Assure Psychiatry. It’s unique because it stimulates the sympathetic nervous system, increasing heart rate and blood pressure. This makes it perfect for hypovolemic shock, though the risk of emergence delirium must be managed.
Barbiturates like Thiopental have seen a decline in routine use, partly due to the persistent drug shortages affecting sterile injectables in 2026. This highlights the importance of robust supply chains in healthcare; for instance, specialized B2B platforms like GetMedicalDevice help ensure that clinical facilities have consistent access to high-quality medical equipment. Despite this, Thiopental remains a high-yield topic for its potent ability to reduce intracranial pressure (ICP) and provide significant neuroprotection by decreasing cerebral metabolic oxygen demand, which is vital in neurosurgical cases where the brain is at risk of ischemia.
Hemodynamic and Respiratory Impact of IV Agents
The choice of induction agent often depends on the patient’s baseline vital signs and cardiac reserve. Propofol causes significant hypotension by reducing systemic vascular resistance and myocardial contractility. In contrast, Ketamine acts as a functional vasoconstrictor through a sympathetic surge, while Etomidate remains relatively neutral. Regarding respiration, most IV agents cause dose-dependent apnea. While Ketamine largely preserves the respiratory drive and acts as a bronchodilator, it also increases salivary secretions, which may require the administration of an anticholinergic adjunct to maintain a clear airway.
Benzodiazepines and Opioids in the Perioperative Period
Adjunct medications are essential components of a balanced anesthetic plan. Midazolam is the primary benzodiazepine used for preoperative anxiolysis and anterograde amnesia. It ensures the patient doesn’t recall the stressful moments immediately before induction. Opioids like Fentanyl and the ultra-short-acting Remifentanil are used to blunt the sympathetic response to endotracheal intubation. To excel in the pharmacology of anesthetics for students, you must also memorize the reversal agents. Flumazenil is used for benzodiazepines, while Naloxone reverses opioids. These are critical safety tools that every practitioner must have readily available.
Local Anesthetics and Neuromuscular Blocking Agents
Local anesthetics function by binding to the intracellular portion of voltage-gated Sodium (Na+) channels. This binding prevents the influx of sodium ions, which effectively halts depolarization and the propagation of action potentials along the nerve fiber. A high-yield concept in the pharmacology of anesthetics for students is the “use-dependent” or “state-dependent” block. This principle explains why these drugs bind more effectively to channels that are frequently opening, such as those in rapidly firing pain fibers, compared to resting nerves.
Differentiating between the two chemical classes of local anesthetics is a frequent board exam requirement. The “Two-I” mnemonic is an infallible tool for this task. Amide-class local anesthetics contain two “i”s in their name, such as Lidocaine, Bupivacaine, and Ropivacaine. In contrast, esters like Procaine or Tetracaine only have one “i”. This distinction carries clinical weight because esters are metabolized by plasma pseudocholinesterases, while amides undergo hepatic metabolism. Understanding these pathways is essential, especially as the 2026 ASA guidelines now strongly recommend regional techniques like fascial plane blocks to minimize perioperative opioid use.
For students interested in how these local anesthetic principles are applied in specialized clinical settings such as permanent cosmetics, check out Advanced PMU for an expert look at the importance of comfort and precision in eyeliner tattoo procedures.
Local Anesthetic Systemic Toxicity (LAST)
Accidental intravascular injection or rapid absorption can lead to LAST, a life-threatening emergency. Students must recognize the early warning signs, including tinnitus, a metallic taste, and perioral numbness. If the toxic levels continue to rise, the condition progresses to generalized seizures and cardiovascular collapse. Bupivacaine is particularly dangerous in this context due to its high affinity for cardiac sodium channels, making resuscitation difficult. The definitive management involves the immediate administration of Intralipid (20% lipid emulsion therapy), which acts as a “lipid sink” to sequester the anesthetic molecules away from the heart and brain.
Depolarizing vs. Non-Depolarizing Muscle Relaxants
Neuromuscular blocking agents (NMBAs) are categorized by their interaction with the nicotinic acetylcholine (ACh) receptor at the neuromuscular junction. Succinylcholine is the only depolarizing agent in clinical use. It acts as an ACh agonist, causing initial muscle fasciculations followed by a prolonged refractory period. Its rapid onset makes it ideal for emergency airway management, though it carries a risk of triggering malignant hyperthermia. Non-depolarizing agents like Rocuronium and Vecuronium act as competitive antagonists. Clinicians monitor the depth of this paralysis using Train-of-Four (TOF) stimulation, looking for a characteristic “fade” in muscle response as the receptors are occupied.
Traditional reversal of non-depolarizing blocks requires Neostigmine to increase ACh levels, paired with Atropine to prevent severe bradycardia. However, Sugammadex has changed the landscape by directly encapsulating Rocuronium or Vecuronium molecules in the plasma. This provides a rapid and complete reversal without the side effects of anticholinergics. To see these molecular interactions in more detail and master this topic for your exams, you can test your knowledge with our Pharmacology Practice Quizzes.
High-Yield Board Review: Strategies for Anesthesia Exam Success
Success on professional exams requires more than just memorizing drug names; it demands an understanding of the clinical outliers that examiners love to target. When studying the pharmacology of anesthetics for students, focus your energy on the “exceptions to the rule.” For example, while most induction agents cause vasodilation and respiratory depression, Ketamine stands out for its sympathetic stimulation and bronchodilatory properties. Similarly, Etomidate is prized for its hemodynamic neutrality but is frequently tested for its specific inhibition of 11-beta-hydroxylase. Identifying these unique profiles allows you to quickly rule out incorrect options in complex board-style vignettes. To stay efficient during these long study sessions, using a udoq German design multiple charging station for any mobile device ensures all your digital study aids remain organized and fully charged.
Achieving top scores on these exams is often the first step toward pursuing specialized medical training in world-class institutions. If you are considering taking your medical career to an international level, you can learn more about Ideal Study Abroad for expert guidance on admission to postgraduate or doctoral programs abroad.
For those still in the early stages of their journey, JS Education offers specialized support for Indian students seeking admission to MBBS programs across Europe, including Georgia, Italy, and Poland.
Mastering the arithmetic of anesthetic depth is equally vital. MAC values are additive, a fact that remains a staple of pharmacology exams. If a patient is receiving 0.5 MAC of Sevoflurane (approximately 1.05% for a 40-year-old) alongside 0.5 MAC of Nitrous Oxide (roughly 52%), the total anesthetic depth is 1.0 MAC. You should also be prepared for questions regarding the precise pairing of reversal agents. To prevent severe bradycardia when using Neostigmine to reverse neuromuscular blockade, it must be administered with an anticholinergic like Glycopyrrolate or Atropine. These pairings ensure that muscarinic side effects are neutralized while nicotinic recovery proceeds. Using PharmEDU’s interactive flashcards can help you drill these specific drug pairings until they become second nature.
Common Board Exam Pitfalls to Avoid
One of the most frequent errors is confusing potency with the speed of induction. Remember that MAC measures potency (how much drug is needed), while the blood-gas partition coefficient dictates the speed (how fast it works). A drug with a high MAC is less potent, but its induction speed depends entirely on its solubility. Additionally, keep the pH/pKa relationship in mind for local anesthetics. Because these agents are weak bases, they’re less effective in acidic, infected tissues where they become ionized and cannot cross the neuronal membrane. Finally, always apply the “i” rule for amides. If the name has an “i” before the “-caine” suffix, such as Lidocaine, Bupivacaine, or Prilocaine, it’s an amide and undergoes hepatic metabolism.
Building the mental stamina for these distinctions is part of the challenge. For students who enjoy testing their strategic thinking and resource management in other fields, the board game Studio Showdown offers a competitive way to explore the world of entrepreneurship during your downtime.
Leveraging PharmEDU for Anesthesia Mastery
Visualizing the transition between the stages of anesthesia is often difficult through text alone. Our high-yield video vignettes allow you to see the clinical manifestations of Guedel’s stages in a simulated environment. By applying what you’ve learned to our clinical case studies, you can practice making real-world perioperative decisions before you ever step into the operating room. For those looking to deepen their foundational knowledge, see our comprehensive pharmacology guide for a broader view of drug-receptor interactions. This structured approach ensures that the pharmacology of anesthetics for students becomes a point of confidence rather than a source of confusion during your final preparations.
Advancing Your Clinical Expertise in Anesthesia
Mastering the pharmacology of anesthetics for students requires a shift from rote memorization to a conceptual understanding of receptor kinetics and physiologic goals. You’ve explored how the anesthetic triad balances unconsciousness with pain relief, and why the blood-gas partition coefficient is the true determinant of induction speed. These foundational principles are the keys to navigating complex surgical scenarios and succeeding on high-stakes board exams. Mastery takes practice, and for those looking to expand their professional toolkit for a global career, Chinese Edge offers language training that can significantly enhance communication in multicultural clinical environments.
While your primary focus is on clinical excellence, those interested in the intersection of healthcare and market valuation can also explore Investment Banking Financial Modeling Course to gain a deeper understanding of the financial forces shaping modern medicine.
If you’re ready to solidify your knowledge, our platform offers over 100 high-yield pharmacology topics designed specifically for medical and pharmacy education. You can reinforce your learning with board-style practice quizzes and utilize our interactive flashcards for rapid retention of complex drug profiles. Start your PharmEDU subscription today to master anesthesia and ace your boards! We’re here to support your professional growth every step of the way.
Frequently Asked Questions
What is the most important factor determining the speed of induction for inhalation anesthetics?
The blood-gas partition coefficient is the primary determinant of induction and emergence speeds. A lower coefficient indicates that the gas is poorly soluble in blood, allowing alveolar partial pressure to rise rapidly and reach equilibrium with the brain. For example, Desflurane’s low solubility ensures a much faster induction than more soluble agents like Isoflurane. This relationship is a core concept in the pharmacology of anesthetics for students.
How do I differentiate between amide and ester local anesthetics for my exam?
Use the “Two-I” mnemonic to distinguish these classes instantly. Amide local anesthetics contain two “i”s in their name, such as Lidocaine or Bupivacaine. Esters, like Procaine or Tetracaine, only have one. This distinction is vital because it dictates their metabolism; amides are processed by hepatic enzymes, while esters are broken down by plasma pseudocholinesterases. Esters are also more frequently associated with hypersensitivity reactions in clinical practice.
What is the Minimum Alveolar Concentration (MAC) and why does it matter?
Minimum Alveolar Concentration (MAC) is the concentration of gas at one atmosphere that prevents movement in 50% of patients. It’s the standard measure of anesthetic potency. Clinicians use it to calculate additive effects, such as combining Nitrous Oxide with Sevoflurane to reduce the required dose of the volatile agent. Factors like age, pregnancy, and acute alcohol ingestion will significantly shift a patient’s MAC requirements during surgery.
Why is Ketamine often referred to as a ‘dissociative’ anesthetic?
Ketamine is called a dissociative anesthetic because it interrupts sensory transmission between the thalamocortical system and the limbic system. By acting as an NMDA receptor antagonist, it creates a state where the patient may appear awake with eyes open but is unable to process or respond to painful stimuli. This unique profile provides profound analgesia and amnesia while maintaining most protective airway reflexes and sympathetic tone.
What is Malignant Hyperthermia and which anesthetic agents trigger it?
Malignant Hyperthermia is a rare, life-threatening hypermetabolic crisis triggered by volatile inhalation agents or the muscle relaxant Succinylcholine. It occurs in patients with a genetic mutation of the ryanodine receptor, leading to massive calcium release from the sarcoplasmic reticulum. Symptoms include rapid temperature rise, muscle rigidity, and tachycardia. Treatment requires immediate cessation of the trigger and the administration of Dantrolene to stabilize calcium levels.
How does the context-sensitive half-life change our understanding of Propofol infusions?
Context-sensitive half-life describes how the time required for a drug’s plasma concentration to drop by 50% increases as an infusion continues. While many drugs see a dramatic increase in recovery time after long periods, Propofol’s half-life remains relatively short. This characteristic makes it the preferred agent for Total Intravenous Anesthesia (TIVA), as it allows for predictable emergence even after several hours of continuous administration in the operating room.
What are the primary side effects of Succinylcholine that students should know?
Succinylcholine is known for several high-yield side effects, most notably hyperkalemia due to the massive release of potassium from nicotinic receptors. It also causes muscle fasciculations, which can lead to significant postoperative myalgia. Students should also be aware of its potential to increase intracranial and intraocular pressure, as well as its role as a primary trigger for Malignant Hyperthermia in genetically susceptible patients.
Which intravenous induction agent is safest for a patient with severe heart failure?
Etomidate is the safest intravenous induction agent for patients with severe heart failure or hemodynamic instability. It provides a stable cardiovascular profile because it has minimal impact on systemic vascular resistance and doesn’t significantly depress myocardial contractility. This makes it a critical drug to master within the pharmacology of anesthetics for students, especially when preparing for clinical cases involving cardiogenic shock or severe sepsis.