Cardiovascular Pharmacology for USMLE: High-Yield Study Guide for 2026
Cardiovascular disease remains the leading cause of death in the United States, accounting for one in every three fatalities. For medical students, mastering cardiovascular pharmacology for USMLE represents more than just a hurdle; it’s a vital clinical foundation that the exam tests with increasing complexity. It’s common to feel overwhelmed when you’re trying to connect drug mechanisms to pressure-volume loops or differentiate between antiarrhythmic classes under the pressure of the new 30-minute exam blocks. You shouldn’t have to rely on isolated buzzwords that fail when a clinical vignette shifts perspective.
This study guide provides a clinical-to-mechanistic review designed to help you master the most frequently tested drug classes and their toxicities. We’ll examine the 2026 ACC/AHA dyslipidemia guidelines, including the new LDL-C goal of less than 55 mg/dL for very high-risk patients, and the recent approval of Baxdrostat for resistant hypertension. By the end of this review, you’ll be able to identify drugs based on specific clinical side effects and confidently select the next best step in management for any cardiovascular scenario. We’ll bridge the gap between basic science and clinical practice to ensure you understand the physiological “why” behind every intervention.
Key Takeaways for USMLE Success
- Learn why cardiovascular pharmacology for USMLE makes up approximately 10 to 15 percent of Step 1 pharmacology questions and how to shift from rote memorization to mechanism-based reasoning.
- Explore the “Big Four” antihypertensive classes and the mechanistic links that allow ACE inhibitors to prevent cardiac remodeling and protect renal function.
- Use the Vaughan Williams classification to simplify Class I through IV antiarrhythmics and understand their specific effects on the action potential slope.
- Identify the four drug classes that improve survival in chronic heart failure and recognize why beta-blockers aren’t used during acute decompensation.
- Implement efficient study habits with PharmEDU’s interactive flashcards and high-yield video vignettes to ensure you don’t just memorize drug lists, but master clinical application.
Mastering Cardiovascular Pharmacology for the USMLE Step 1 and Step 2
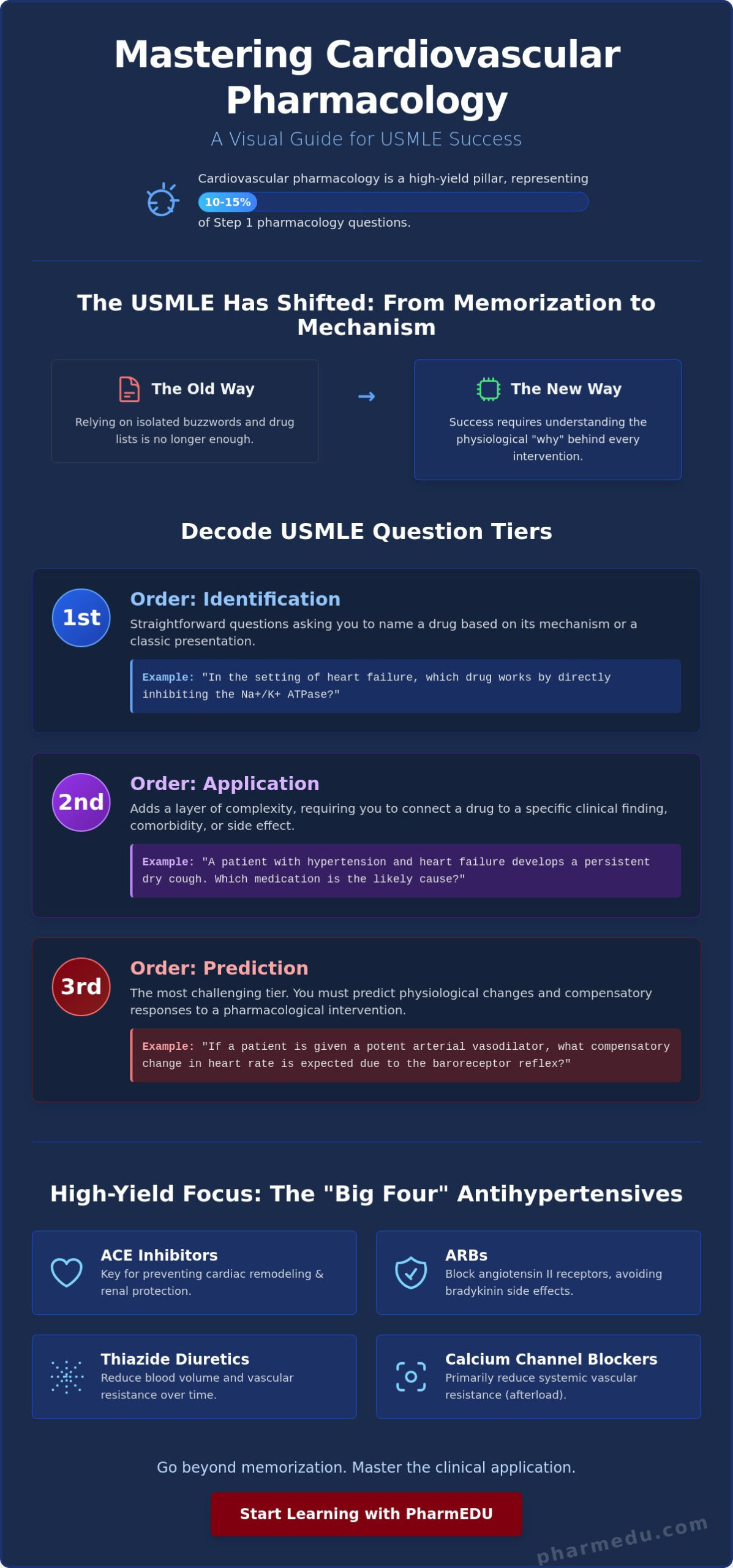
Cardiovascular pharmacology for USMLE isn’t just another subject; it’s a high-yield pillar that appears in roughly 10-15% of Step 1 pharmacology questions. The USMLE has shifted away from simple recall. In 2026, you’re expected to demonstrate mechanism-based clinical reasoning. This means you must understand how a drug interacts with a patient’s physiology rather than just knowing its name. High-yield focus areas include antihypertensives, antiarrhythmics, and heart failure management. If you don’t understand the “why” behind the drug, you’ll struggle when the vignette adds a comorbidity like renal failure or asthma.
The USMLE Testing Style: 1st, 2nd, and 3rd-Order Questions
The exam uses a tiered approach to test your knowledge. You’ll need to move beyond simple identification to succeed in the updated 2026 exam format. The questions generally fall into three categories:
- 1st-Order: These are straightforward identification questions. They might ask you to name a drug based on a mechanistic description, such as inhibiting the Na+/K+ ATPase in the setting of heart failure.
- 2nd-Order: These add a layer of complexity. You might need to identify a specific toxicity, like a “dry cough” or “angioedema,” based on a drug prescribed for a patient with a specific condition like hypertension.
- 3rd-Order: These are the most challenging. They require you to predict physiological changes. For example, if a patient is given a potent vasodilator, you must predict the resulting change in heart rate or cardiac output due to compensatory mechanisms.
This level of reasoning is exactly what our clinical case studies are designed to build. It’s about seeing the patient profile and predicting the outcome before you even look at the answer choices.
Core Autonomic Integration
You can’t master heart medications without a firm grasp of the autonomic nervous system. Receptors like Alpha-1, Beta-1, and Beta-2 are the switches that control the cardiovascular system. If you’re looking for a solid foundation before diving into specific agents, our Pharmacology: The Comprehensive Guide to the Science of Drugs provides the necessary background. Understanding these receptors is a non-negotiable prerequisite.
The baroreceptor reflex is a frequent source of confusion. It often complicates pharmacological interventions by triggering reflex tachycardia when blood pressure drops. To keep these classes organized, you might review a comprehensive list of cardiac pharmaceutical agents to see how they’re categorized by their primary autonomic or ionic targets. This structural understanding helps you navigate clinical vignettes where multiple receptors are involved.
With the 2026 USMLE software updates introducing shorter 30-minute blocks, your ability to quickly integrate ANS physiology with drug mechanisms is vital. There’s less time to second-guess your logic. Mastering these interactions allows you to answer questions about why certain drugs, like hydralazine, are almost always paired with a beta-blocker to prevent compensatory heart rate spikes. You’re not just learning a list; you’re learning the language of hemodynamics.
Antihypertensive Agents: Mechanistic Links to Hemodynamics
Hypertension management in 2026 centers on the “Big Four” drug classes: ACE inhibitors, ARBs, Thiazide diuretics, and Calcium Channel Blockers. Success in cardiovascular pharmacology for USMLE requires you to look past drug names and focus on how these agents alter the pressure-volume loop. For example, dihydropyridines primarily reduce systemic vascular resistance, which lowers afterload and shifts the loop to the left. You can explore these hemodynamic interactions further at Cardiovascular Pharmacology Concepts, where the relationship between resistance and cardiac work is explained in detail.
ACE Inhibitors and ARBs: The Renal Connection
ACE inhibitors and ARBs are high-yield because of their specific impact on renal hemodynamics. By inhibiting the production or action of Angiotensin II, these drugs preferentially dilate the efferent arteriole. This reduces the intraglomerular pressure, which is why they’re the first-line choice for nephroprotection in patients with diabetes. However, this same mechanism can cause a transient rise in serum creatinine. You’ll likely see questions focusing on the classic triad of side effects: hyperkalemia, angioedema, and a dry, non-productive cough caused by bradykinin accumulation. For a deeper dive into these specific pathways, our guide on ACE Inhibitors Pharmacology breaks down the latest 2026 clinical data.
Calcium Channel Blockers: Dihydropyridines vs. Non-Dihydropyridines
Calcium channel blockers (CCBs) are divided by their selectivity. Dihydropyridines like amlodipine and nifedipine act on vascular smooth muscle L-type channels. They’re primarily used for hypertension and Raynaud’s phenomenon. Nimodipine is a specific high-yield DHP used to prevent cerebral vasospasm following a subarachnoid hemorrhage. In contrast, non-dihydropyridines like verapamil and diltiazem are more cardiac-selective. They’re used for rate control in supraventricular tachycardias but carry a risk of bradycardia or heart block. Common toxicities to remember include peripheral edema and gingival hyperplasia.
Diuretics require you to visualize the nephron. Thiazides act on the distal convoluted tubule and are “calcium-sparing,” which makes them useful for hypertensive patients with osteoporosis. Loop diuretics, however, inhibit the Na+/K+/2Cl- cotransporter in the thick ascending limb and lead to “calcium-wasting.” Both classes can cause hypokalemia, a frequent distractor in cardiovascular pharmacology for USMLE questions. To see how these electrolyte shifts manifest in patient scenarios, our Clinical Case Studies provide an excellent way to practice your diagnostic skills before exam day. With the 2026 approval of Baxdrostat, a first-in-class aldosterone synthase inhibitor, understanding the RAAS system has never been more relevant for managing resistant hypertension.
The Antiarrhythmic Framework: Simplifying Class I-IV Agents
Antiarrhythmic agents often represent the most daunting chapter in cardiovascular pharmacology for USMLE. To master these, you’ve got to move beyond a list of names and visualize the cardiac action potential. The Vaughan Williams classification remains the gold standard for exam preparation because it organizes drugs by their primary electrophysiological effect. Whether you’re analyzing a rhythm strip or predicting a drug’s effect on the QT interval, this framework is your most reliable tool. You’ll find a detailed overview of cardiovascular drugs helpful for seeing how these classes fit into broader treatment algorithms for atrial fibrillation.
Class I Subclasses: The “Double Science” Mnemonic
Class I drugs are sodium channel blockers that primarily affect Phase 0 depolarization. The exam frequently tests your ability to distinguish between the three subclasses based on their binding kinetics and effect on the action potential (AP) duration. Class Ia agents, such as Procainamide and Quinidine, lengthen the AP duration. In contrast, Class Ib agents like Lidocaine shorten it. They specifically target ischemic or depolarized tissue, making them high-yield choices for post-myocardial infarction arrhythmias. Class Ic drugs, including Flecainide, have the strongest binding affinity. They don’t change the AP duration but significantly widen the QRS complex. If you’re struggling to keep these straight, our Interactive Pharmacology Flashcards use comparative clinical scenarios to cement these differences.
Amiodarone: The “Swiss Army Knife” with High Toxicity
Amiodarone is a unique agent. While it’s officially categorized as Class III, it actually possesses Class I, II, and IV properties. This versatility makes it incredibly effective for both atrial and ventricular arrhythmias, but it comes at a high cost of multi-organ toxicity. For the USMLE, you must recognize the specific buzzword side effects that point directly to this drug. These include pulmonary fibrosis, a blue-gray skin discoloration often called “Smurf skin,” and both hyper- and hypothyroidism due to its high iodine content. Because of its long half-life and extensive tissue distribution, patients require rigorous monitoring. You’ll need to know the necessary baseline and follow-up tests: Pulmonary Function Tests (PFTs), Liver Function Tests (LFTs), and Thyroid Function Tests (TFTs).
Class III agents like Sotalol and Dofetilide block potassium channels, prolonging Phase 3 repolarization. This increases the QT interval, which carries a significant risk of inducing Torsades de Pointes. Managing the AV node for rate control usually involves Class II (Beta-blockers) or Class IV (Calcium channel blockers like Verapamil). These agents prolong the PR interval by slowing conduction through the node. Understanding these ionic shifts is vital for answering 3rd-order questions about EKG changes. Our High-Yield Video Vignettes break down these action potential shifts visually, ensuring you don’t just memorize the classes but actually understand the electrophysiology behind them.
High-Yield Clinical Scenarios: Heart Failure and Ischemic Heart Disease
Clinical vignettes often require you to choose the “next best step” in management, a task that tests your ability to prioritize interventions. In the context of cardiovascular pharmacology for USMLE, you must distinguish between therapies that provide symptomatic relief and those that offer a proven mortality benefit. This distinction is most critical in heart failure. While loop diuretics are essential for managing fluid overload in acute decompensated heart failure, they don’t improve long-term survival. Conversely, beta-blockers are a cornerstone of chronic management but are strictly contraindicated during an acute flare because their negative inotropic effects can worsen a patient’s hemodynamic status.
Drugs that Improve Mortality in Heart Failure
For chronic heart failure with reduced ejection fraction (HFrEF), four specific drug classes are your high-yield targets for survival improvement. These include:
- ACE Inhibitors or ARBs: These reduce afterload and prevent cardiac remodeling.
- Beta-blockers: Specifically Carvedilol, Bisoprolol, and Metoprolol succinate.
- Mineralocorticoid Receptor Antagonists: Spironolactone or eplerenone, which block the fibrotic effects of aldosterone.
- Hydralazine and Isosorbide Dinitrate: This combination is particularly effective in African American populations with HFrEF.
The 2026 approval of Baxdrostat has introduced new discussions around aldosterone synthase inhibition, though it’s currently focused on resistant hypertension. You’ll need to keep these survival-improving agents straight to correctly answer management questions. If you want to practice these distinctions under exam-like conditions, our Pharmacology Practice Quizzes allow you to test your knowledge against realistic clinical scenarios.
Acute Coronary Syndrome (ACS) Management
The classic “MONA” mnemonic (Morphine, Oxygen, Nitrates, Aspirin) has evolved in the 2026 guidelines. While aspirin remains the immediate first step, the use of morphine and oxygen is now more selective, reserved for patients with refractory pain or hypoxia. In the setting of an ST-elevation MI (STEMI), the priority is reperfusion. You’ll be asked to choose between primary percutaneous coronary intervention (PCI) and thrombolytics. PCI is the gold standard if available within 90 to 120 minutes of first medical contact. Thrombolytics like Alteplase are reserved for when PCI isn’t an option, provided there are no absolute contraindications like a history of intracranial hemorrhage.
Managing ischemic heart disease also involves long-term lipid control. The March 2026 guidelines have reintroduced specific LDL-C goals, setting a target of less than 55 mg/dL for very high-risk patients with ASCVD. This shift toward aggressive management makes understanding statin mechanisms and their side effects, like myopathy and hepatotoxicity, even more relevant. For those also preparing for pharmacy board exams, our The Best NAPLEX Prep Course Guide provides additional context on how these clinical guidelines translate into pharmacy practice.
Anti-anginal therapy often features questions about nitrates and beta-blockers. Nitrates primarily cause venodilation, which reduces preload and cardiac work. A classic USMLE “buzzword” is “Monday Disease.” This refers to industrial workers exposed to nitroglycerin who develop a tolerance during the week, only to experience “rebound” symptoms like headaches and tachycardia when they return to work on Monday after a weekend away from the exposure. Understanding these physiological nuances is what separates a passing score from a top-tier result in cardiovascular pharmacology for USMLE.
Efficient Study Strategies: From Rote Memorization to Clinical Mastery
Success on the USMLE requires more than just a passing familiarity with drug names. With the 2026 application fees for Step 1 and Step 2 CK set at $695 each, you want to ensure your preparation is as efficient as possible. Rote memorization often fails when you’re faced with complex clinical vignettes. Instead, you must adopt active recall and spaced repetition. These techniques force your brain to retrieve information, which strengthens neural pathways and ensures that cardiovascular pharmacology for USMLE becomes second nature. Identifying your blind spots in cardiovascular physiology is much easier when you’re consistently testing yourself rather than just highlighting a text.
PharmEDU: Your High-Yield Digital Mentor
Our platform is designed to act as a digital mentor, guiding you through the intricacies of drug interactions and hemodynamic shifts. We offer micro-learning segments that fit perfectly into the gaps of a busy clinical rotation. Our interactive pharmacology practice quizzes mimic the updated 2026 USMLE interface, which now features 30-minute blocks. This helps you build the necessary speed and stamina for the 14 blocks of Step 1 or 16 blocks of Step 2 CK. If you’re still weighing your study options, our guide on Comprehensive Pharmacy Review: Digital Platforms vs. Textbooks explains why modern digital tools are outpacing traditional methods in 2026.
Building a 4-Week Cardiovascular Review Plan
A structured approach prevents you from feeling overwhelmed by the volume of information. We recommend a four-week deep dive to master cardiovascular pharmacology for USMLE:
- Week 1: Autonomics and Hemodynamics. Focus on receptor profiles and how they influence the pressure-volume loop.
- Week 2: Antihypertensives and Diuretics. Master the “Big Four” and the electrolyte shifts associated with each diuretic class.
- Week 3: Antiarrhythmics and Inotropes. Use our high-yield video vignettes to visualize action potential changes and the Vaughan Williams classification.
- Week 4: Clinical Integrated Cases and Toxicities. Spend this week on our interactive pharmacology flashcards to drill those buzzword toxicities like Amiodarone’s thyroid effects or Digoxin’s yellow-tinted vision.
Practice questions are your most valuable diagnostic tool. They reveal exactly where your understanding of the physiological “why” breaks down. By integrating clinical case studies into your daily routine, you move beyond memorizing lists and start thinking like a clinician. This transition is essential for correctly answering the “next best step in management” questions that dominate the current exam landscape. Our goal is to take the administrative and cognitive burden off your shoulders, allowing you to focus on continuous professional growth and exam success. Our annual and monthly subscriptions provide the flexibility you need to stay on track during your study period.
Elevate Your Clinical Reasoning for 2026
Mastering cardiovascular pharmacology for USMLE is a journey from simple memorization to sophisticated clinical reasoning. You’ve explored how antihypertensives alter hemodynamics, decoded the complexities of the Vaughan Williams classification, and identified the specific drug classes that improve survival in heart failure. These concepts are the foundation of your future practice. By focusing on the physiological “why” rather than just drug names, you prepare yourself for the most challenging 3rd-order questions on the exam.
To ensure you’re fully prepared for the updated 2026 exam format, you need tools that match the rigor of the boards. PharmEDU offers over 100 high-yield topics through mobile-compliant micro-learning segments that fit into your busy schedule. You can reinforce your knowledge with interactive flashcards and clinical case studies designed to bridge the gap between theory and practice. Master USMLE Pharmacology with PharmEDU High-Yield Vignettes and transform your study routine into a path toward clinical mastery. Your dedication to understanding these mechanisms today will lead to better patient outcomes tomorrow. You’ve got the tools; now it’s time to apply them with confidence.
Frequently Asked Questions
What are the most high-yield cardiovascular drugs for USMLE Step 1?
The most high-yield cardiovascular pharmacology for USMLE topics focus on ACE inhibitors, loop diuretics, statins, and beta-blockers. These classes are frequently tested because they form the foundational management for hypertension, heart failure, and myocardial infarction. You’ll need to master their specific effects on hemodynamics and electrolyte balances rather than just memorizing their names. Understanding how these agents alter the pressure-volume loop is essential for answering third-order questions correctly.
How do I remember the Class I antiarrhythmic subgroups?
You can remember Class I antiarrhythmics by their binding affinity to sodium channels and their effect on the action potential duration. Class Ia has intermediate binding, Class Ib has the weakest binding, and Class Ic has the strongest binding. This explains why Class Ic causes the most significant QRS widening. While Class Ia lengthens the action potential, Class Ib shortens it, and Class Ic has no significant effect on the duration itself.
Which heart failure medications actually decrease mortality?
In chronic heart failure, the medications proven to decrease mortality include ACE inhibitors, ARBs, and specific beta-blockers like carvedilol, bisoprolol, and metoprolol succinate. Mineralocorticoid receptor antagonists like spironolactone also provide a survival benefit. It’s important to remember that while loop diuretics are vital for symptomatic relief and fluid management, they haven’t been shown to reduce long-term mortality in these patients.
What is the “buzzword” for Amiodarone toxicity on the USMLE?
The primary buzzwords for Amiodarone toxicity you’ll encounter are “pulmonary fibrosis,” “blue-gray skin discoloration,” and “thyroid dysfunction.” Since the drug contains significant amounts of iodine, it can trigger either hyperthyroidism or hypothyroidism. You’ll also likely see questions regarding its exceptionally long half-life and the requirement for baseline monitoring of pulmonary, liver, and thyroid functions before starting a patient on the medication.
How do ACE inhibitors cause a dry cough?
ACE inhibitors cause a dry cough by preventing the breakdown of bradykinin and substance P in the lungs. When these pro-inflammatory peptides accumulate, they sensitize the sensory neurons in the airways. If a patient develops this side effect, it’s a common exam scenario to ask for the next best step, which is switching the patient to an ARB. ARBs don’t affect bradykinin levels, so they don’t cause the cough.
What is the difference between Dihydropyridine and Non-Dihydropyridine CCBs?
Dihydropyridines like amlodipine act primarily on vascular smooth muscle to cause vasodilation and reduce afterload. Non-dihydropyridines like verapamil and diltiazem act directly on the heart to decrease contractility and slow conduction through the AV node. This makes non-DHPs useful for rate control in atrial fibrillation, but they’re generally avoided in patients with heart failure due to their negative inotropic effects.
Can I use Beta-blockers in acute decompensated heart failure?
You shouldn’t use beta-blockers during an acute decompensated heart failure flare. Their negative inotropic effect can further decrease cardiac output in a patient who’s already struggling with hemodynamic stability. In a clinical vignette, you’ll wait until the patient is stable and “dry” on diuretic therapy before starting or up-titrating a beta-blocker. Mastering these timing nuances is a key part of cardiovascular pharmacology for USMLE preparation.
What is Cinchonism and which drug causes it?
Cinchonism is a syndrome characterized by tinnitus, headache, and dizziness, and it’s classically caused by the Class Ia antiarrhythmic Quinidine. It’s a favorite high-yield fact for examiners focusing on drug toxicities. If a patient presents with these specific neurological symptoms after starting a medication for an arrhythmia, Quinidine is the likely culprit. You should also watch for other side effects like thrombocytopenia or a prolonged QT interval.
Similar Posts
Pharmacology: The Comprehensive Guide to the Science of Drugs
What if the 1,500+ FDA-approved drugs currently available were actually just variations of a few core molecular patterns? It’s no secret that the…
Pharmacology Video Lectures for Nursing Students: The 2026 Guide to High-Yield Learning
What if the secret to passing your toughest nursing course isn’t more hours in the library, but a shift in how you process clinical data? With nearly…
Autonomic Nervous System Pharmacology Review: High-Yield Guide for 2026
With nearly 50% of hypertension patients in the United States failing to reach their blood pressure goals despite multiple treatments, the…
Respiratory Pharmacology for NCLEX: The High-Yield 2026 Study Guide
With the NCLEX-RN first-time pass rate for U.S. educated candidates reaching 86.8% in early 2026, the pressure to master complex clinical judgment…
Pharmacology of Diuretics Made Easy: The High-Yield Study Guide (2026)
What if mastering the pharmacology of diuretics wasn’t about brute-force memorization, but simply visualizing five specific checkpoints along the…
Antimicrobial Pharmacology High Yield: The 2026 Board Review Guide
Memorizing every single antibiotic in the pharmacopeia is the fastest way to fail your 2026 boards. You’re likely feeling the weight of information…