Common Medication Errors to Avoid: A 2026 Clinical Safety Guide
Did you know that preventable medication errors in U.S. hospitals now cost between $20 and $40 billion every single year? For healthcare professionals, mastering the common medication errors to avoid is more than a clinical requirement; it’s a fundamental commitment to patient safety in an increasingly complex environment. You’ve likely felt that sharp spike of anxiety when faced with similar-sounding drug names or complex dosing for high-alert medications. It’s a heavy burden to carry, especially when you’re also striving to excel on the NAPLEX or NCLEX exams where safety scores are paramount.
We understand that safety is a clinical skill rooted in deep pharmacological knowledge, not just a simple checklist. This 2026 guide provides the systematic frameworks and pharmacological insights you need to identify, prevent, and eliminate errors before they reach the patient. We’ll examine the Joint Commission’s National Performance Goals effective January 1, 2026, and dive into the specific high-risk scenarios identified in the latest ISMP best practices. By the end of this article, you’ll have the safety-first mindset and technical expertise required to lead your team with confidence and precision.
Key Takeaways
- Identify the critical differences between prescribing, dispensing, and administration errors to strengthen every link in the medication use process.
- Navigate the updated 2026 ISMP List of Confused Drug Names to implement effective safeguards against Look-Alike/Sound-Alike (LASA) drug confusion.
- Master the specialized pharmacological protocols for high-alert medications, specifically focusing on the “Big Three”: insulin, anticoagulants, and opioids.
- Utilize Reason’s Swiss Cheese Model and advanced CPOE frameworks to systematically eliminate common medication errors to avoid in your clinical practice.
- Develop the safety-first clinical mindset required to achieve high scores on the safety and error prevention domains of the NAPLEX and NCLEX exams.
Understanding Medication Errors: Definitions and Clinical Impact
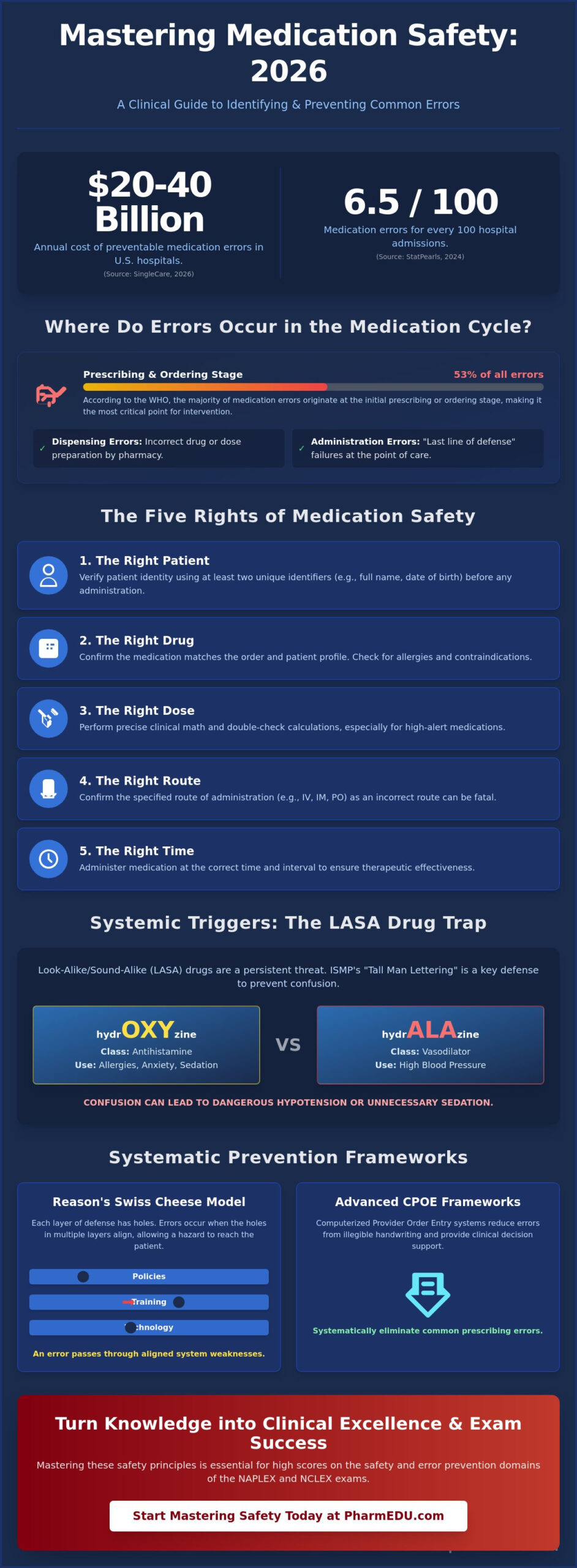
Medication errors represent any preventable event that may lead to inappropriate medication use or patient harm while the drug is in the control of the healthcare professional or patient. Understanding these failures is the first step in identifying common medication errors to avoid in clinical settings. According to 2026 data from SingleCare, these preventable adverse drug events (ADEs) cost U.S. hospitals between $20 and $40 billion annually. This Medical Error Overview highlights that while many mistakes are systemic, the clinical impact is deeply personal, often resulting in extended hospital stays or, in tragic cases, patient fatalities. StatPearls reported in 2024 that hospital settings see approximately 6.5 medication errors for every 100 admissions, making precision a non-negotiable skill for modern practitioners.
The Taxonomy of Error: Prescribing vs. Administration
Prescribing errors occur when a clinician selects the wrong drug or provides an illegible order, often serving as the initial point of failure in the medication cycle. Data from the WHO in 2024 indicates that 53% of all medication errors happen during this prescribing or ordering stage. Administration errors represent a different challenge because they happen at the point of care, where the nurse or technician acts as the last line of defense. When a failure occurs here, there’s no remaining safety net to catch the mistake. We also track ‘near misses,’ which are errors that were caught before reaching the patient. These events provide invaluable data for improving clinical protocols without causing actual harm.
The Five Rights of Medication Safety
The ‘Five Rights’ framework remains the foundational safety standard for preventing common medication errors to avoid. It requires a disciplined approach to every single dose. Adhering to these principles ensures that pharmacological interventions remain therapeutic rather than hazardous.
- Right Patient: Use at least two unique identifiers, such as the patient’s full name and date of birth, to ensure the medication matches the individual. This step is critical in preventing misidentification errors in busy clinical environments.
- Right Drug: Cross-reference the medication order with the patient’s current pharmacology profile. This practice helps identify potential contraindications or allergies before the drug is prepared.
- Right Dose, Route, and Time: This involves precise clinical math and attention to detail. Administering a drug via the wrong route or at the wrong interval can turn a therapeutic intervention into a toxic one. For example, a drug intended for oral use administered intravenously can be fatal.
Mastering these basics isn’t just about passing the NCLEX or NAPLEX with high safety scores. It’s about building a professional habit that protects lives every day. By internalizing these definitions and frameworks, you transition from simply following instructions to becoming an active guardian of patient safety.
Systemic Triggers: LASA Drugs and Communication Failures
Systemic triggers often hide in plain sight, waiting for a lapse in concentration to manifest as a clinical failure. Look-alike/sound-alike (LASA) drugs remain a persistent threat to patient safety. The Institute for Safe Medication Practices (ISMP) released its 2026-2027 Targeted Medication Safety Best Practices, emphasizing that visual and auditory confusion accounts for a significant portion of preventable events. Tall Man Lettering, a technique that uses capitalized letters to highlight differences in drug names, has become a standard visual defense. As discussed in the AHRQ on Medication Errors primer, these systemic failures require more than just individual vigilance; they demand robust institutional protocols to protect patients from common medication errors to avoid.
The LASA Trap: Common Drug Name Confusions
In clinical practice, confusing hydrOXYzine with hydrALAzine can lead to dangerous hypotensive episodes or unnecessary sedation. This is why a deep understanding of pharmacology is essential for distinguishing between drug classes that sound similar but function differently. Indication-based prescribing, where the prescriber includes the purpose of the medication on the order, serves as a secondary check. If a pharmacist sees a drug prescribed for hypertension but the drug name matches an antihistamine, the error is caught before dispensing. These are the types of common medication errors to avoid through proactive pharmacological review and systematic double-checks.
Verbal Orders and Dangerous Abbreviations
Communication breakdowns often stem from verbal orders or the use of ambiguous abbreviations. The Joint Commission’s National Performance Goals, effective January 1, 2026, continue to discourage verbal orders except in emergencies. When they must occur, the “Read-Back” technique is mandatory. The clinician receiving the order must write it down and read it back to the prescriber to confirm accuracy. Additionally, avoiding the “Do Not Use” list is vital. Symbols like “U” for units or “QD” for daily are frequently misread, leading to tenfold dosing errors or incorrect frequencies that can compromise therapy.
Technology has significantly reduced these risks by standardizing how we communicate. By 2025, 90% of hospitals adopted Computerized Physician Order Entry (CPOE) systems, which automatically flag dangerous abbreviations and LASA drug pairs. While software provides a safety net, your personal knowledge remains the primary defense mechanism. Utilizing tools like interactive pharmacology flashcards can help you internalize these drug name differences and safety protocols, ensuring you’re prepared for both board exams and high-pressure clinical shifts where communication must be flawless.
High-alert medications represent a specific class of drugs that carry a heightened risk of causing significant patient harm when used incorrectly. While mistakes may not be more frequent with these agents, the consequences of a failure are often devastating. Understanding the common causes of medication error involving these substances is a critical competency for any clinical practitioner. Many of these drugs have a Narrow Therapeutic Index (NTI). This means the difference between a therapeutic dose and a toxic one is dangerously small. To mitigate this risk, healthcare systems implement independent double-checks. This is a process where two clinicians verify the drug, dose, and patient separately to ensure accuracy. It’s one of the most effective strategies for identifying common medication errors to avoid before they reach the bedside.
Insulin and Anticoagulants: The Precision Challenge
Insulin is the most frequently reported high-alert medication involved in errors within acute care settings, primarily due to the complexity of sliding scales and confusion between various insulin types. When managing these patients, clinicians must also consider drug-drug interactions. For instance, ACE inhibitors can occasionally potentiate the hypoglycemic effects of insulin or mask certain symptoms of low blood sugar, which complicates the clinical picture. Anticoagulants like Heparin and Warfarin present a different precision challenge. These drugs require rigorous monitoring of laboratory values like aPTT and PT/INR to prevent life-threatening hemorrhages. In 2026, the Joint Commission’s National Performance Goals explicitly emphasize taking extra care with patients on blood thinners, reflecting their status as a top safety priority.
Opioids and Sedatives: Respiratory Depression Risks
Opioids and sedatives pose a severe risk due to their potential to induce respiratory depression. Patient-controlled analgesia (PCA) pumps offer a technological solution for pain management, but they aren’t foolproof. Errors in programming these devices or “PCA by proxy” can lead to oversedation. Clinical monitoring must focus on the rate and depth of respiration rather than just pulse oximetry. Oxygen saturation can remain normal even while a patient is hypoventilating. Safety protocols must include immediate access to pharmacological reversal agents. Naloxone is the standard for opioid overdose; Flumazenil is utilized for benzodiazepine reversal. By mastering the monitoring requirements for these agents, you can effectively reduce the common medication errors to avoid in post-operative or intensive care units.
Prevention Frameworks: From the Swiss Cheese Model to CPOE
James Reason’s Swiss Cheese Model provides a vital lens for understanding how common medication errors to avoid actually happen. Instead of blaming a single clinician, this model views safety as a series of defensive layers. Each layer, from the pharmacist’s initial review to the nurse’s bedside check, has potential “holes” or weaknesses. When these holes align, an error reaches the patient. Strengthening these layers involves integrating advanced technology like Computerized Physician Order Entry (CPOE) and Clinical Decision Support (CDS). By 2025, 90% of hospitals had successfully adopted CPOE systems to catch prescribing mistakes at the source. These digital tools provide real-time alerts for allergies and drug interactions, acting as a primary barrier against systemic failure.
Barcode Medication Administration (BCMA) serves as an additional safety net, with 93% of hospitals meeting adoption standards by 2025. However, technology only works within a “Just Culture.” This framework encourages professionals to report errors and “near misses” without fear of retribution, focusing on system improvements rather than individual punishment. This transparency is essential for long-term clinical safety. To master these clinical safety frameworks and prepare for your boards, explore our Institutional Platform License for comprehensive team training.
Institutional Safety Technology
Modern hospitals rely on “Smart Pumps” equipped with Dose-Error Reduction Systems (DERS) to prevent infusion rate errors. These devices use pre-programmed drug libraries to ensure dosages stay within safe limits. Automated dispensing cabinets (ADCs) also streamline the pharmacy workflow by limiting access to specific medications. A major challenge in 2026 is “alert fatigue.” This occurs when clinicians are overwhelmed by constant software warnings, leading them to bypass critical safety checks. Staying vigilant requires a balance between trusting the digital system and maintaining high-level professional oversight.
The Role of Patient Education in Error Prevention
Patient involvement is a powerful, often underutilized, defense mechanism. Teaching patients the “Brown Bag Review,” where they bring all current medications to an appointment for reconciliation, helps catch discrepancies during transitions of care. Counseling on drug-food interactions, such as the effect of grapefruit juice on certain statins, further prevents adverse events. Ensuring patients understand the purpose of their therapy is easier when clinicians utilize a comprehensive pharmacology study guide for nursing students to prepare for these educational interactions. By empowering the patient, we add one final, critical layer to the Swiss Cheese Model.
Mastering Safety for Board Exams: The PharmEDU Advantage
Boards in 2026 don’t just test what you know; they test how safely you can apply that knowledge in a high-stakes environment. The NAPLEX and NCLEX have significantly increased the weighting of safety-related competencies to reflect modern clinical demands. For instance, the Pharmacy Technician Certification Board (PTCB) 2026 syllabus update now weights federal requirements and regulatory compliance at 18.75%, up from 12.5% in previous years. To excel on these exams, you must identify common medication errors to avoid by applying deep pharmacological insights rather than relying on simple checklists. Knowledge-based errors often stem from a lack of understanding regarding drug-drug interactions or narrow therapeutic indices. PharmEDU’s high-yield video vignettes simulate these high-pressure scenarios, helping you build the clinical intuition necessary to protect your future patients.
High-Yield Safety Topics for the NAPLEX
Calculations remain a primary hurdle for many candidates, particularly when dealing with complex sterile compounding or pediatric dosing. A single misplaced decimal point can result in a tenfold overdose, which is a catastrophic safety failure. Our naplex prep course integrates safety protocols into every drug class review, from oncology to cardiovascular health. Mastering dose conversions is a fundamental skill that prevents the mathematical errors frequently seen in clinical practice. By focusing on these high-yield areas, you ensure that your board preparation aligns with the latest 2026 safety standards.
Developing Clinical Judgment with PharmEDU
Building clinical intuition takes time and consistent, focused practice. Utilizing interactive pharmacology flashcards allows you to memorize LASA pairs and high-alert protocols through active recall. This method is far more effective than passive reading for internalizing the nuances of drug names like hydrOXYzine and hydrALAzine. We also emphasize micro-learning as a core strategy. By studying in short bursts, you avoid the cognitive fatigue that leads to 53% of prescribing errors. This systematic approach builds a safety-first mindset that lasts long after you’ve received your license. Join PharmEDU today to master the comprehensive pharmacy review needed for a safe and prosperous career.
Cultivating a Safety-First Clinical Mindset
Clinical safety is a dynamic skill that evolves alongside new regulations and pharmacological discoveries. By mastering the common medication errors to avoid, you transition from a passive participant to an active guardian of patient health. This journey requires a deep understanding of high-alert medication protocols and a commitment to the systemic defense layers outlined in modern safety frameworks. Whether you’re preparing for board exams or managing a complex ward, your precision is the ultimate safety net for those in your care.
Refining this expertise doesn’t have to be an administrative burden. PharmEDU provides a mobile-compliant micro-learning design used by top US nursing and pharmacy schools to streamline your professional development. With access to over 100 high-yield pharmacology topics, you can build the clinical intuition needed to excel in 2026 and beyond. Master pharmacology safety with a PharmEDU subscription today and join a community dedicated to clinical excellence. Your commitment to continuous learning is the most powerful tool in preventing patient harm.
Frequently Asked Questions
What is the most common medication error in nursing?
Administration errors, specifically wrong-time errors and omitted doses, occur most frequently at the bedside. While prescribing accounts for 53% of total mistakes across the system, the nurse represents the final barrier before a drug reaches the patient. Identifying these common medication errors to avoid requires absolute adherence to barcode scanning protocols. In 2025, 93% of hospitals met BCMA standards to address this specific vulnerability in the nursing workflow.
How can I remember Look-Alike/Sound-Alike drug names?
Utilize Tall Man Lettering and indication-based prescribing to create visual and cognitive distinctions between similar names. For example, differentiating buPROPion from busPIRone prevents pharmacological mix-ups during the dispensing process. ISMP’s 2026 updates suggest storing LASA drugs in separate, labeled bins within automated dispensing cabinets. These physical barriers force a “stop and think” moment that overrides the brain’s tendency to see what it expects to see.
What are the ‘Five Rights’ of medication administration?
The ‘Five Rights’ include the right patient, drug, dose, route, and time. This framework ensures that every clinical intervention follows a standardized safety path. While simple, these steps are the primary defense against the common medication errors to avoid in high-pressure environments. Modern systems often add “Right Documentation” and “Right Reason” to provide a more comprehensive 2026 clinical safety profile for practitioners.
What medications are considered ‘High-Alert’?
High-alert medications include any drugs that bear a heightened risk of causing significant patient harm when used in error. Beyond the standard insulin and anticoagulants, the 2026 ISMP list emphasizes concentrated electrolytes and intravenous push medications. These substances require independent double-checks because their pharmacological effects are often immediate and irreversible. Mastering the narrow therapeutic index of these agents is essential for safe clinical practice.
How does the Swiss Cheese Model apply to medication errors?
The Swiss Cheese Model posits that errors occur when multiple small failures align across different organizational layers. In a hospital, these “holes” might include an illegible prescription, a distracted pharmacist, and a failed barcode scanner. When these gaps line up, the error reaches the patient. Safety strategies focus on closing these holes through better communication, technology, and a supportive institutional culture that prioritizes patient well-being over blame.
Can technology completely eliminate medication errors?
Technology serves as a powerful safety net but cannot eliminate the human element of clinical care. Systems like CPOE and smart pumps catch many mistakes, yet they also introduce new risks like alert fatigue and technical workarounds. By 2026, healthcare leaders recognized that technology must be paired with deep pharmacological knowledge. Professional vigilance remains the most effective tool for preventing errors that software might overlook during a busy shift.
What should I do if I witness a medication error?
Immediate priority must be given to the patient’s clinical status and physical safety. Once the patient is stabilized, you must report the event through your institution’s formal error-reporting system. This process isn’t about finger-pointing; it’s about the “Just Culture” where data is used to prevent future failures. Prompt reporting allows the medical team to implement reversal protocols or increased monitoring to mitigate potential harm to the patient.
How are medication safety questions formatted on the NAPLEX?
NAPLEX safety questions often appear as case-based scenarios or “select-all-that-apply” (SATA) formats. You might be asked to identify a prescribing error in a patient profile or select the correct counseling points for a high-alert medication. These questions test your ability to recognize contraindications and perform precise calculations under pressure. High safety scores on these boards demonstrate that you possess the clinical judgment required for a responsible pharmacy career.