Pediatric Pharmacology Dosage Considerations: The High-Yield Clinical Guide
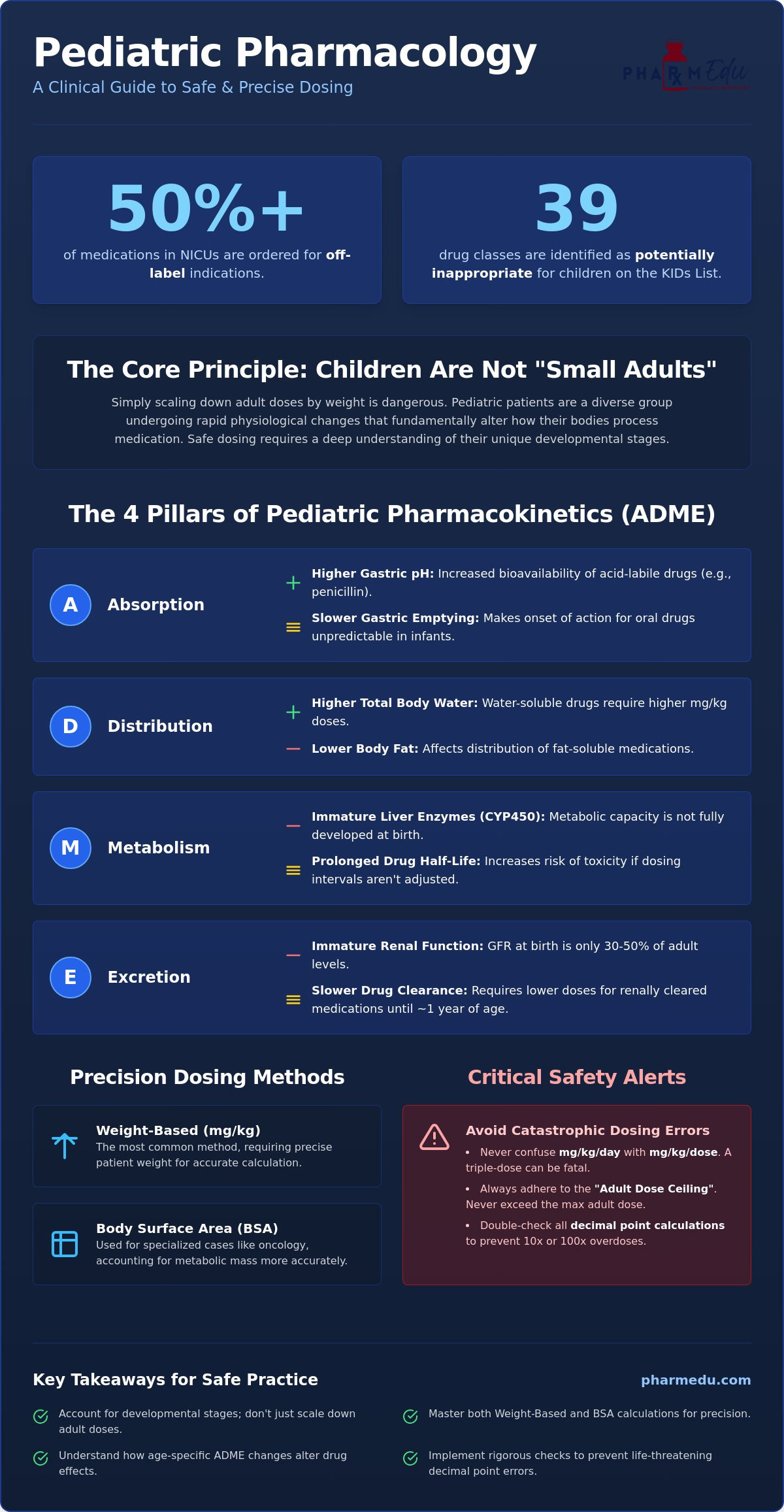
Did you know that in neonatal intensive care units, over 50% of all medications ordered are for off-label indications? This startling statistic from 2025 highlights why pediatric pharmacology dosage considerations aren’t just a subset of adult medicine, but a distinct and high-stakes clinical discipline. When you’re dealing with a population where the latest KIDs List identifies 39 drug classes as potentially inappropriate, the margin for error remains razor thin.
It’s natural to feel a sense of trepidation when shifting from standardized adult dosing to complex weight-based or body surface area calculations. We understand the pressure of avoiding decimal point errors while accounting for how a child’s developing organs metabolize drugs. This guide will help you master these critical physiological factors, ensuring you can calculate doses with absolute precision and pass your pharmacology board exams with high-yield knowledge. We’ll explore essential ADME differences across age groups, the impact of current drug shortages, and the practical strategies needed to provide safe, evidence-based care.
Key Takeaways
- Understand why pediatric patients require a unique clinical approach that accounts for developmental stages rather than simply scaling down adult doses.
- Master the nuances of weight-based versus body surface area calculations to ensure precise administration in specialized cases like oncology.
- Gain high-yield insights into how age-specific physiological changes, such as blood-brain barrier permeability in neonates, fundamentally alter drug distribution.
- Learn to implement the “5 Rights” and rigorous rounding strategies to navigate complex pediatric pharmacology dosage considerations and prevent life-threatening decimal point errors.
- Discover how to leverage High-Yield Video Vignettes and interactive tools to streamline your study process for pharmacology board exams.
Understanding the “Not Small Adults” Principle in Pediatric Dosing
The “Not Small Adults” principle is the cornerstone of clinical pediatrics. It’s a fundamental shift in perspective that recognizes pediatric patients as a heterogeneous group undergoing rapid physiological evolution. You can’t simply take an adult dose and scale it down based on weight alone. Doing so ignores the complex developmental milestones that dictate how a body interacts with medication. This biological reality is why pediatric pharmacology dosage considerations are so critical for clinical safety and patient outcomes.
For decades, children were frequently categorized as “therapeutic orphans.” Most drugs were developed and tested exclusively on adults, leaving clinicians to prescribe off-label without the benefit of robust pediatric clinical trial data. While regulatory frameworks like the Best Pharmaceuticals for Children Act (BPCA) and the Pediatric Research Equity Act (PREA) have successfully incentivized pediatric labeling, the gap in data remains a challenge. Understanding Pediatric Physiology is essential because children aren’t just smaller; they’re biologically distinct at every stage of growth from the neonatal period through adolescence.
The Four Pillars of Pediatric Pharmacokinetics (ADME)
Pharmacokinetics describes what the body does to a drug. In children, this process is highly dynamic and changes as organs mature. These shifts directly influence pediatric pharmacology dosage considerations at the bedside.
- Absorption: Neonates have a higher gastric pH (less acidic) than adults, which significantly increases the bioavailability of acid-labile drugs like penicillin. Gastric emptying is also slower and irregular in infancy, making the onset of action for many oral medications unpredictable.
- Distribution: Infants possess a much higher percentage of total body water and lower body fat than adults. Water-soluble drugs like gentamicin require higher mg/kg doses to reach therapeutic levels because they distribute into a larger volume of fluid relative to their size.
- Metabolism: The liver’s metabolic capacity isn’t fully developed at birth. Specifically, cytochrome P450 (CYP450) enzymes mature at different rates. This can lead to a significantly prolonged drug half-life, increasing the risk of toxicity if dosing intervals aren’t carefully adjusted.
- Excretion: Renal function is immature in neonates. The Glomerular Filtration Rate (GFR) is only about 30% to 50% of adult levels at birth and doesn’t reach adult capacity until roughly one year of age, requiring lower doses for renally cleared medications.
Pharmacodynamics: Why Response Differs
While pharmacokinetics deals with drug movement, pharmacodynamics focuses on the drug’s effect on the body. Pediatric patients often show different receptor sensitivity or density compared to adults. This variability explains why a child might experience a paradoxical reaction, such as becoming hyperactive after receiving diphenhydramine instead of feeling drowsy. Mastering pharmacology fundamentals allows you to predict these unique responses rather than reacting to them after an error occurs. Clinical success depends on recognizing that a child’s biological targets are moving targets.
Calculating Pediatric Dosages: Weight-Based vs. BSA Methods
Precision in calculation is the primary defense against medication errors in children. While adult dosing often relies on standardized amounts, pediatric pharmacology dosage considerations require a more granular approach. Most clinicians utilize either weight-based or Body Surface Area (BSA) methods. Regardless of the method chosen, you must always adhere to the “Adult Dose Ceiling” rule. If your calculated pediatric dose exceeds the maximum recommended adult dose, you must cap the prescription at the adult limit to prevent toxicity.
One of the most frequent errors in clinical practice involves confusing “mg/kg/day” with “mg/kg/dose.” A prescription for 30 mg/kg/day divided into three doses means the child receives 10 mg/kg per administration. Administering the full 30 mg/kg three times a day would result in a triple dose, potentially leading to catastrophic outcomes. While modern practice favors these specific calculations, historical Pediatric Dosage Calculation Methods like Clark’s Rule still provide foundational context for how weight-based dosing evolved.
Weight-Based Dosing: The Gold Standard
Weight-based dosing is the most common method used in general pediatrics. The first step is always obtaining an accurate weight in kilograms. Since many parents still report weight in pounds, you’ll need to divide by 2.2 to convert. Accuracy matters. A small error in conversion scales quickly. For obese pediatric patients, the calculation becomes more complex. Using actual body weight for hydrophilic drugs can lead to overdosing, so clinicians often use ideal body weight or an adjusted weight to ensure safety. Refining these skills through Clinical Case Studies can help bridge the gap between theory and safe practice.
Body Surface Area (BSA) and Nomograms
BSA is often considered a more accurate reflection of a patient’s metabolic activity and physiological state than weight alone. It’s the preferred method for high-yield drug classes with narrow therapeutic indices, such as chemotherapy agents and certain antiretrovirals. To calculate this, clinicians often use the Mosteller formula. This formula defines BSA as the square root of the product of height in centimeters and weight in kilograms, divided by 3,600. In fast-paced clinical settings, the West Nomogram remains a vital tool. By drawing a straight line between the child’s height and weight on the chart, you can quickly determine the BSA in square meters. This method accounts for the fact that metabolic rates are more closely tied to surface area than simple mass, providing a safer profile for highly toxic medications.
Developmental Milestones and Age-Specific Dosing Considerations
Clinical success in pediatrics requires moving beyond a single “child” category. The pediatric spectrum spans from the fragile neonate to the near adult adolescent, each representing a unique physiological stage. Because organ systems develop at different rates, pediatric pharmacology dosage considerations must be adjusted as the child grows. A dose that’s safe for a school age child could be toxic for a neonate due to differences in blood-brain barrier permeability. In newborns, this barrier is more porous, allowing CNS active drugs like morphine to reach higher concentrations in the brain than they would in older patients.
Age specific toxicities often stem from a child’s inability to process certain excipients. A classic example is “Gasping Syndrome,” a potentially fatal condition caused by benzyl alcohol. While adults easily metabolize this preservative, neonates lack the necessary enzyme pathways, leading to metabolic acidosis and respiratory failure. Ensuring Medication Safety in Children involves constant vigilance regarding these hidden components in drug formulations.
Neonatal and Infant Considerations
The first months of life present the most significant metabolic hurdles. Immature glucuronidation pathways in the liver mean neonates can’t conjugate certain drugs efficiently. This was tragically demonstrated by “Gray Baby Syndrome,” where the antibiotic chloramphenicol accumulated to toxic levels. Additionally, infants have a much thinner stratum corneum. This leads to increased percutaneous absorption, meaning topical medications can quickly reach systemic levels and cause unintended side effects. You must also account for protein binding. Sulfonamides, for example, can displace bilirubin from albumin, increasing the risk of kernicterus in newborns.
The Toddler and School-Age Peak
Interestingly, toddlers often represent a metabolic peak. Between ages one and three, children frequently require higher relative doses of medications like theophylline or phenytoin because their hepatic metabolism and renal clearance are remarkably rapid. During this stage, the challenge often shifts from physiology to adherence. Palatability is a major factor in success. Choosing the right dosage form, such as a flavored liquid versus a chewable tablet, can determine whether a treatment plan succeeds. Caregivers are your primary partners here. Educating them on how to measure doses accurately using oral syringes rather than household spoons is a vital step in preventing errors at home.
Adolescent Challenges
As patients enter adolescence, hormonal changes and growth spurts introduce new variables. Puberty can alter drug metabolism and body composition, sometimes necessitating a transition toward adult dosing strategies. However, clinicians must remain cautious. Even an adolescent who physically resembles an adult may still have developing cognitive functions that affect their ability to manage complex medication schedules independently.
Medication Safety: Preventing Errors and Dose Rounding Strategies
The “Ten-Fold Error” remains one of the most dangerous risks in pediatric care. A simple misplaced decimal point transforms a therapeutic dose into a lethal one, turning 0.1 mg into 1.0 mg in an instant. This risk is amplified in children because their smaller body mass offers no buffer against toxicity. To mitigate this, clinicians must rigorously apply the “5 Rights” of medication administration: the right patient, drug, dose, route, and time. In the pediatric context, the “right dose” is often the most complex to verify. The most common cause of pediatric medication errors is dosing miscalculations.
Dose rounding is a practical strategy used to bridge the gap between theoretical math and clinical administration. For most medications with a wide therapeutic index, rounding within a 5% to 10% range is acceptable. If a calculation results in 4.92 mg, rounding to 5 mg allows for accurate measurement in an oral syringe. This reduces the risk of a caregiver or nurse struggling to measure an impossible volume. These pediatric pharmacology dosage considerations require a balance between mathematical precision and the practical realities of the bedside.
Standardization and Ready-to-Use (RTU) Medications
Standardized concentrations and Ready-to-Use (RTU) formulations are vital for reducing cognitive load. When pharmacy departments provide pre-mixed concentrations, they remove the need for complex bedside math during high-stress emergencies. While this works well for school-age children, it presents unique challenges in neonatal settings. Neonates often require such minute volumes that even standardized concentrations may be too dilute for their strict fluid limits, requiring highly specific, customized pharmacy preparations.
The Role of Technology in Dosing Safety
Technology has introduced powerful safeguards like Computerized Provider Order Entry (CPOE). These systems provide real-time alerts if a dose falls outside the expected weight-based range for a patient’s age. Similarly, smart pumps utilize “soft limits” that warn a nurse of unusual entries and “hard limits” that stop the pump from running at dangerous rates. Despite these advances, manual double-checks remain essential. Technology can be bypassed or suffer from “alert fatigue,” but a second pair of trained eyes remains the final line of defense. You can sharpen your error-detection skills by working through our Clinical Case Studies, which highlight real-world safety scenarios and help you practice these critical checks.
Mastering Pediatric Pharmacology with PharmEDU
Translating theory into clinical practice is the most significant hurdle for students and new clinicians. While understanding pediatric pharmacology dosage considerations is essential for safety, memorizing the myriad of weight-based ranges and developmental nuances can feel overwhelming. PharmEDU serves as a digital mentor, providing the structured, high-yield resources you need to manage these complexities with confidence. Our High-Yield Video Vignettes break down intricate ADME concepts into manageable insights, ensuring you understand the biological “why” behind every dose adjustment.
Memorization is only half the battle; application is where true mastery begins. By using our Interactive Pharmacology Flashcards, you can drill weight-based dosing ranges for the most common pediatric drugs until they become second nature. This active recall strategy is particularly effective when used alongside our pharmacology study guide for nursing students. This integrated approach ensures that whether you’re at the bedside or in the classroom, your knowledge remains sharp and practical.
High-Yield Review for Board Exams
Success on the NAPLEX or NCLEX requires more than just knowing drug names. You must be able to solve multi-step calculation questions under intense exam pressure. PharmEDU’s Pharmacology Practice Quizzes simulate these high-stakes environments, focusing on the pediatric drug classes most frequently tested. We provide specific tools to refine your approach:
- Identify high-yield pediatric drug classes to prioritize your study hours effectively.
- Master the conversion between pounds and kilograms with rapid, error-free techniques.
- Practice differentiating between mg/kg/day and mg/kg/dose to eliminate common calculation traps.
Our Clinical Case Studies bridge the gap between classroom learning and clinical reality, offering scenarios that test your ability to apply pediatric pharmacology dosage considerations in a simulated environment. This prepares you to transition from a cautious student to a precise, confident clinician.
Subscription Benefits for Busy Students
We recognize that medical and nursing students have demanding schedules. Our platform is built for efficiency, featuring micro-learning segments that fit perfectly into the gaps between clinical rotations. Whether you choose a PharmEDU Monthly Subscription or a PharmEDU Annual Subscription, you’ll gain mobile-compliant access to our entire library. This allows you to review critical dosing guidelines or watch a quick vignette on the go, ensuring your professional development never pauses. Excel in your pharmacology coursework with a PharmEDU subscription today.
Advancing Patient Safety with Pediatric Expertise
Mastering the nuances of child-specific medicine requires a definitive move away from the “small adult” mindset. By focusing on developmental ADME changes and utilizing precise calculation methods like Body Surface Area when necessary, you protect your most vulnerable patients from adverse events. Safety isn’t just about the math; it’s about understanding why a neonate responds differently than an adolescent and maintaining a rigorous commitment to the “5 Rights” during every clinical interaction.
Navigating complex pediatric pharmacology dosage considerations is a career-long journey that begins with a solid educational foundation. PharmEDU provides the high-yield tools you need to bridge the gap between classroom theory and clinical excellence. Our platform features over 100 High-Yield Pharmacology Topics and Interactive Practice Quizzes designed by healthcare educators to help you succeed on board exams and in daily practice. Master Pediatric Pharmacology with PharmEDU today. Your dedication to precision and continuous learning ensures a safer future for every child in your care.
Frequently Asked Questions
What is the most common method for calculating pediatric doses?
Weight-based dosing, expressed in milligrams per kilogram (mg/kg), is the most common method for calculating pediatric doses. This approach ensures that the medication amount scales with the child’s body mass rather than using a standardized adult amount. It’s essential to obtain an accurate weight in kilograms to avoid conversion errors. Clinicians must always cross-check the final result against the maximum recommended adult dose to ensure the “adult ceiling” isn’t exceeded.
Why is the Body Surface Area (BSA) method sometimes preferred over weight-based dosing?
The Body Surface Area (BSA) method is preferred for medications with a narrow therapeutic index, such as chemotherapy or certain antiretrovirals, because it more accurately reflects metabolic activity. While weight only measures mass, BSA accounts for physiological maturity and fluid distribution. Clinicians typically use the Mosteller formula or a West Nomogram to determine BSA in square meters. This precision is vital when managing pediatric pharmacology dosage considerations for high-toxicity drug classes.
How does gastric pH in neonates affect drug absorption?
Neonates have a higher gastric pH, meaning their stomachs are less acidic than those of older children or adults. This alkalinity increases the absorption of acid-labile medications, such as penicillin, which would otherwise be degraded in a more acidic environment. Conversely, it can delay or decrease the absorption of weak acids. These shifts in absorption necessitate careful timing and dosage adjustments during the first few weeks of life when the gastrointestinal tract is still maturing.
What is a 10-fold dosing error and how can it be prevented?
A 10-fold dosing error occurs when a misplaced decimal point causes a patient to receive ten times the intended dose. This is the most dangerous type of miscalculation in pediatrics because children have very little physiological buffer against toxicity. To prevent this, always use a leading zero for doses less than one (e.g., 0.5 mg) and never use a trailing zero (e.g., use 5 mg, not 5.0 mg). Manual double-checks by a second clinician remain the gold standard for safety.
Are there specific drugs that are contraindicated in pediatric patients due to developmental risks?
Several drugs are restricted in children, such as tetracyclines, which can cause permanent tooth discoloration in patients under eight years old. The 2025 KIDs List also advises against using codeine in children under 12 due to the risk of fatal respiratory depression. Additionally, fluoroquinolones are generally avoided in pediatric patients because of potential risks to developing bone and cartilage, unless no other therapeutic options exist for a specific, severe infection.
How do I calculate a pediatric dose if only the adult dose is known?
If only the adult dose is known, historical formulas like Clark’s Rule (Weight in lbs / 150 x Adult Dose) can provide an estimate, but they aren’t the standard in modern practice. The safest approach is to consult a dedicated pediatric pharmacopeia or the FDA-approved labeling for pediatric-specific data. Relying solely on adult dose extrapolation is risky because pediatric pharmacology dosage considerations must account for the fact that children’s pharmacokinetics don’t scale linearly with weight.
What role does the liver play in pediatric drug metabolism maturation?
The liver is the primary site for drug metabolism, but its enzyme systems, particularly the Cytochrome P450 (CYP450) family, are immature at birth. This reduced metabolic capacity means that many drugs have a significantly longer half-life in neonates, requiring longer dosing intervals to avoid accumulation. For example, immature glucuronidation pathways can lead to toxic levels of certain antibiotics. Liver function typically reaches adult-like capacity by the end of the first year of life.
Can I round a pediatric dose to the nearest whole number?
You can round a pediatric dose to a measurable whole number if the change falls within a safe range, typically 5% to 10% of the calculated total. This is often necessary to allow for practical administration using an oral syringe or standardized tablet sizes. However, rounding is not appropriate for high-potency drugs with narrow therapeutic windows. In those critical cases, the exact calculated dose must be maintained to avoid subtherapeutic levels or unintended toxicity.