Common Drug Interactions Study Guide: High-Yield Pharmacology Review for 2026
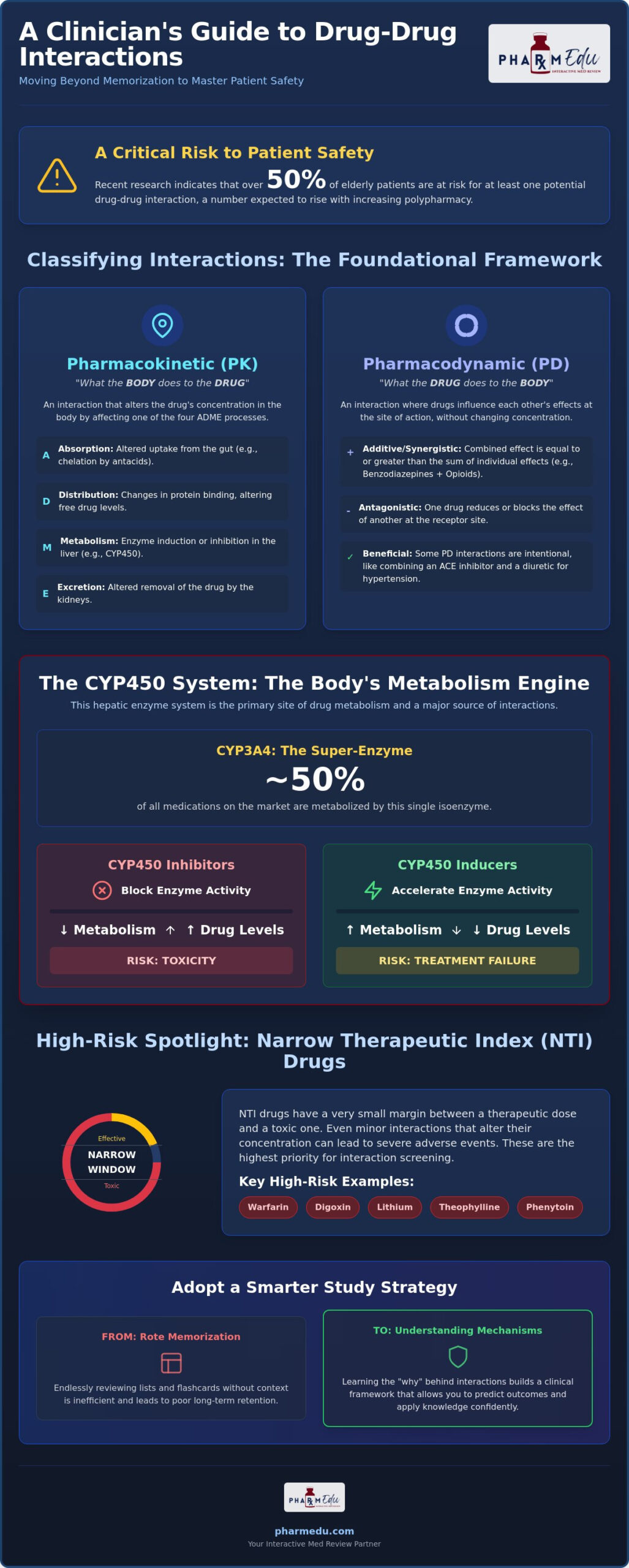
Recent 2024 research indicates that over 50% of elderly patients are currently at risk for at least one potential drug-drug interaction. With polypharmacy rates rising and the FDA approving dozens of new small molecule drugs in 2025, the volume of clinical data is staggering. You’ve likely spent nights staring at endless tables of CYP450 inducers, fearing you’ll miss a critical red flag on a board exam. It’s exhausting to memorize lists when you don’t fully grasp the underlying mechanisms. This common drug interactions study guide is designed to replace that confusion with a clear, logical framework.
We’ll help you master the clinical significance of high-yield drug pairs by focusing on the physiological “why” rather than just the “what.” You’ll learn to distinguish between complex pharmacokinetic and pharmacodynamic pathways with ease. By the end of this review, you’ll have the tools to apply the latest ICH M12 regulatory standards and FDA labeling updates to real-world scenarios. This approach builds the genuine confidence you need to excel in your pharmacology coursework and dominate your 2026 board exams.
Key Takeaways
- Develop a clinical framework to distinguish between pharmacokinetic and pharmacodynamic mechanisms, allowing you to predict how drugs interact within the body.
- Master the Cytochrome P450 system by identifying potent inducers and inhibitors that directly impact drug serum levels and patient safety.
- Prioritize the “Big 5” Narrow Therapeutic Index drugs, including Warfarin and Digoxin, which represent the highest risk for clinically significant interactions.
- Utilize this common drug interactions study guide to recognize high-yield “red flag” drug pairs frequently featured on NAPLEX and NCLEX board exams.
- Transition from rote memorization to a structured study strategy that emphasizes understanding the “why” behind interactions for better long-term retention.
Classifying Drug-Drug Interactions (DDIs): PK vs. PD Mechanisms
A clinically significant drug-drug interaction (DDI) occurs when the pharmacological or toxicological effect of one medication is modified by the co-administration of another substance. While many students treat these events as isolated facts to memorize, this common drug interactions study guide emphasizes that DDIs are predictable based on physiological principles. To master this topic, you must first identify the specific roles within the interaction. The “object” drug is the medication whose effect is being changed, while the “precipitant” drug is the agent causing the change. By categorizing these events into pharmacokinetic or pharmacodynamic mechanisms, you can move beyond simple flashcards and start thinking like a clinician. This Drug interaction overview provides a foundational look at how these categories separate the body’s handling of a drug from the drug’s effect on the body.
Understanding the mechanism is superior to rote memorization because it allows you to predict interactions for entire drug classes rather than individual agents. When you know how a drug is processed, you can anticipate potential “red flags” before they appear on a patient’s chart or an exam paper. This logical approach reduces the fear of missing a critical interaction during high-stakes board exams or clinical rotations.
Pharmacokinetic (PK) Interactions: Absorption to Excretion
Pharmacokinetic interactions involve changes in the ADME process, which stands for absorption, distribution, metabolism, and excretion. These occur when a precipitant drug alters the concentration of the object drug in the systemic circulation. Absorption is often the first point of conflict. For instance, antacids that increase gastric pH or cause chelation can significantly reduce the bioavailability of tetracyclines or fluoroquinolones. Competitive protein displacement increases the free, active fraction of highly protein-bound drugs in the plasma, which can lead to sudden toxicity even if total drug levels appear normal. Metabolism and excretion follow similar logic, where the induction or inhibition of enzymes and transporters dictates how long a drug remains active in the system.
Pharmacodynamic (PD) Interactions: Receptor-Level Events
Pharmacodynamic interactions happen at the site of action, typically at the receptor level, without necessarily changing the drug’s plasma concentration. These are often classified as additive, synergistic, or antagonistic. Additive effects occur when two drugs with similar actions produce a combined effect equal to the sum of their individual parts. Synergism goes further, creating a combined effect greater than the sum. While many interactions are dangerous, some are clinically intentional. Combining ACE inhibitors with diuretics is a beneficial strategy to manage hypertension through complementary physiological pathways. Conversely, the risk of overlapping toxicities is high when patients receive multiple CNS depressants, such as benzodiazepines and opioids, which can lead to life-threatening respiratory depression. Mastering these receptor-level events is a core component of this common drug interactions study guide because it highlights the direct impact on patient safety.
The CYP450 System: Mastering Inducers and Inhibitors
The Cytochrome P450 (CYP450) enzyme system acts as the primary engine for hepatic drug metabolism. For any student using a common drug interactions study guide, understanding this system is non-negotiable. While dozens of isoenzymes exist, CYP3A4 remains the most clinically significant enzyme because it metabolizes approximately 50% of all medications currently on the market. Beyond the liver, we must also consider P-glycoprotein (P-gp). This efflux transporter often works in tandem with CYP3A4, pumping drugs out of enterocytes back into the gut lumen, which further complicates the pharmacokinetic profile of many oral medications. When a drug alters these systems, the clinical consequences can be life-threatening.
The clinical impact depends on whether a co-administered drug acts as an inhibitor or an inducer. Inhibitors block enzyme activity, leading to increased serum levels of the object drug and a significantly higher risk of toxicity. Conversely, inducers stimulate the production of more enzymes, which accelerates metabolism and often results in subtherapeutic drug levels and treatment failure. These Clinically Relevant Drug-Drug Interactions require constant vigilance, especially when managing patients on polypharmacy regimens. Mastering these concepts is simpler when you apply them to real-world scenarios, such as those found in our Clinical Case Studies.
Major CYP450 Inhibitors: The ‘SICKFACES.COM’ Mnemonic
Inhibition typically occurs rapidly, often within 24 to 48 hours of starting the precipitant drug. This fast onset makes inhibitors particularly dangerous when paired with Narrow Therapeutic Index (NTI) drugs, as serum levels can spike before the next dose. You can remember the major inhibitors using the SICKFACES.COM mnemonic:
- Sodium Valproate
- Isoniazid
- Cimetidine
- Ketoconazole (and other azoles)
- Fluoxetine
- Alcohol (acute use)
- Chloramphenicol
- Erythromycin (and macrolides, except azithromycin)
- Sulfonamides
- Ciprofloxacin
- Omeprazole
- Metronidazole
- Grapefruit Juice
Major CYP450 Inducers: The ‘PS-PORCS’ Mnemonic
Unlike inhibitors, inducers have a delayed effect because they require the synthesis of new enzyme proteins. This process can take several days or even weeks to reach a steady state, and the effect persists for a similar duration after the inducer is stopped. Rifampin is considered a universal inducer because it potently activates the pregnane X receptor, triggering the massive up-regulation of almost all major CYP isoenzymes and drug transporters. To keep these straight during an exam, use the PS-PORCS mnemonic:
- Phenytoin
- Smoking
- Phenobarbital
- Oxcarbazepine
- Rifampin
- Carbamazepine
- St. John’s Wort
Narrow Therapeutic Index (NTI) Drugs: The High-Risk Targets
Drugs with a Narrow Therapeutic Index (NTI) are the most frequent “object” drugs in clinical practice. This means the margin between a therapeutic dose and a toxic dose is razor-thin. In any common drug interactions study guide, these medications deserve priority because a small change in their systemic concentration can lead to catastrophic clinical outcomes. Unlike drugs with a wide therapeutic window, NTI agents require consistent Therapeutic Drug Monitoring (TDM) to ensure serum levels remain within a specific, safe range. Beyond hepatic metabolism, P-glycoprotein (P-gp) acts as a critical gatekeeper for many NTI drugs. When a precipitant drug inhibits P-gp, it can cause the systemic concentration of the NTI drug to skyrocket, even if the dose remains unchanged.
The “Big 5” NTI medications that appear most frequently on board exams include Warfarin, Digoxin, Lithium, Theophylline, and Phenytoin. Mastering these targets is about more than just remembering names. It’s about understanding the specific physiological triggers that push a patient from a stable state into a toxic crisis. Whether it’s a change in renal clearance, an electrolyte shift, or an enzyme inhibition event, the result is often a “red flag” scenario that requires immediate intervention.
Warfarin: The King of Drug Interactions
Warfarin is notoriously difficult to manage because it relies heavily on the CYP2C9 enzyme and is sensitive to dietary Vitamin K. While consistency in diet is important, the most dangerous interactions involve the “FAB-4” precipitant drugs: Fluconazole, Amiodarone, Bactrim, and Flagyl (Metronidazole). These agents potently inhibit the metabolism of Warfarin, causing the International Normalized Ratio (INR) to spike. Clinicians must monitor PT/INR levels closely and often preemptively reduce the Warfarin dose when starting these medications to prevent life-threatening bleeding events.
Digoxin and Lithium: Electrolyte-Driven Interactions
Not all interactions are enzyme-based; some are driven by electrolyte imbalances and renal clearance. Digoxin toxicity is a classic example. Since potassium and digoxin compete for the same binding site on the Na+/K+ ATPase pump, hypokalemia (often caused by loop diuretics) increases the risk of Digoxin binding and subsequent toxicity. Watch for vignettes describing yellow-green vision or arrhythmias. Lithium follows a similar renal-dependent path. Since the kidneys process lithium much like sodium, drugs that decrease lithium clearance, such as NSAIDs and ACE inhibitors, can lead to toxic accumulation. This common drug interactions study guide highlights coarse tremors and ataxia as the primary clinical signs of lithium toxicity to watch for during exams.
High-Yield ‘Red Flag’ Pairs for Board Exams (NAPLEX & NCLEX)
Board exams like the NAPLEX and NCLEX don’t just test your ability to recognize drug names; they evaluate your capacity to prevent life-threatening errors. These “never-ever” combinations are high-yield because the clinical consequences are immediate and severe. While this common drug interactions study guide provides a broad clinical framework, students should refer to our specialized pharmacology study guide for nursing students for class-specific administration protocols. Mastering these red flags ensures you can identify a dangerous prescription before it ever reaches the patient.
Serotonin Syndrome and QT Prolongation
Serotonin syndrome is a classic board exam topic that results from excessive serotonergic activity in the central nervous system. This typically occurs when patients combine SSRIs with MAOIs without a proper washout period, or when adding triptans for migraine management. You’ll need to recognize symptoms like hyperreflexia, clonus, and hyperthermia in clinical vignettes. Another critical cardiovascular red flag is QT prolongation. When agents like fluoroquinolones, macrolides, and certain antipsychotics are used together, the additive effect on the heart’s electrical cycle increases the risk of Torsades de Pointes. This lethal arrhythmia requires immediate intervention, making these pairings essential to memorize for any high-stakes exam.
The Bleeding Risk: Anticoagulants + Antiplatelets + NSAIDs
Bleeding risks often involve a pharmacodynamic synergy where the medications don’t necessarily change each other’s blood levels but amplify the physiological effect. Combining warfarin with aspirin or NSAIDs significantly compromises hemostasis and gastric mucosal integrity. You must also account for herbal supplements, specifically the “G” herbs: ginger, ginkgo, garlic, and ginseng. These can independently increase bleeding risk and are frequently hidden in patient-purchased supplements. Pharmacists must screen for OTC NSAID use in anticoagulated patients to prevent occult gastrointestinal bleeding that often goes unnoticed until it becomes a crisis.
Identifying these patterns in a split second is what separates top-tier candidates from the rest. If you want to challenge your ability to spot these interactions under pressure, try our Pharmacology Practice Quizzes to refine your clinical judgment before exam day.
How to Master Drug Interactions in Your Study Plan
Mastering drug-drug interactions isn’t about memorizing a thousand individual pairs. It’s about developing a clinical instinct for how drug classes behave. Instead of staring at dry tables, you should transition to high-yield pharmacology review methods that prioritize physiological mechanisms. The most effective approach is the ‘One Class at a Time’ strategy. By focusing on the core metabolic pathways of a single drug class before moving to the next, you build a solid foundation for long-term retention. This common drug interactions study guide serves as your roadmap, but real mastery comes from applying this knowledge to clinical case studies where you must identify “red flags” in a patient’s history.
Utilizing PharmEDU’s Micro-Learning Platform
Active recall is the gold standard for medical education. Our platform is built to facilitate this through targeted, efficient tools. High-Yield Video Vignettes break down complex CYP450 pathways into digestible visual lessons, making it easier to visualize enzyme inhibition and induction. You can then reinforce these concepts using Interactive Pharmacology Flashcards, which are designed for repetitive DDI testing. To ensure you’re ready for the actual exam environment, our practice quizzes mimic the exact formats used in NAPLEX and NCLEX. This structured progression ensures you don’t just recognize a drug name, but you understand its clinical impact.
Creating Your Own DDI Matrix
Visual learners often benefit from creating a DDI matrix. Build a grid that maps major drug classes against common precipitant factors like CYP3A4 inhibitors or renal clearance competitors. This visual representation helps you see the “big picture” and identify patterns across seemingly unrelated medications. Once your matrix is complete, try the Feynman technique. Teaching these concepts to a peer is the ultimate check for mastery. If you can explain why Rifampin lowers the efficacy of oral contraceptives without looking at your notes, you’ve moved past rote memorization into true clinical understanding. This common drug interactions study guide is just the beginning of your journey. To take your preparation to the next level, join PharmEDU to access our full library of pharmacology review topics and secure your success in 2026.
Elevate Your Clinical Practice and Board Readiness
Mastering drug interactions is a cornerstone of patient safety and a non-negotiable skill for any future clinician. By shifting your focus from rote memorization to understanding the physiological “why” of pharmacokinetic and pharmacodynamic mechanisms, you transform a complex subject into a manageable framework. This common drug interactions study guide has highlighted the critical importance of the CYP450 system and the high stakes involved with Narrow Therapeutic Index drugs. Whether you’re navigating clinical rotations or preparing for 2026 board exams, recognizing these red flags is essential for protecting your patients and ensuring your professional success.
We’ve built the tools to help you reach this level of mastery with precision and confidence. Our platform features over 100 High-Yield Video Vignettes that simplify drug metabolism, alongside Interactive Flashcards for Active Recall and NAPLEX & NCLEX-Aligned Practice Quizzes. You don’t have to face these academic challenges alone. Start Your PharmEDU Subscription Today and Master Pharmacology to gain the practical knowledge you need for the next step in your medical career. We’re here to support your professional growth every step of the way.
Frequently Asked Questions
What is the difference between an inducer and an inhibitor in drug interactions?
An inducer increases the activity of metabolic enzymes, which accelerates the breakdown of other medications and typically results in subtherapeutic levels. In contrast, an inhibitor slows down enzyme activity, causing “object” drugs to accumulate in the system and increasing the risk of toxicity. This distinction is a fundamental concept in any common drug interactions study guide, as the onset of inhibition is usually much faster than the gradual process of enzyme induction.
Which foods are most likely to cause clinically significant drug interactions?
High-risk dietary interactions often involve Vitamin K-rich leafy greens, which can antagonize the effects of warfarin, and tyramine-containing foods like aged cheeses or cured meats that trigger hypertensive crises in patients on MAOIs. Additionally, dairy products and calcium supplements can chelate with certain antibiotics, such as tetracyclines and fluoroquinolones. This process significantly reduces their absorption in the gut and can lead to treatment failure if patients aren’t properly counseled on administration timing.
How do I identify a narrow therapeutic index (NTI) drug?
You can identify a Narrow Therapeutic Index (NTI) drug by checking if it requires routine Therapeutic Drug Monitoring (TDM) to ensure serum levels remain within a specific range. Clinically, these drugs are defined by having a small margin between their effective dose and their toxic dose. If a medication’s labeling suggests that even a twofold change in blood concentration could result in serious adverse events or subtherapeutic effects, it’s categorized as an NTI agent.
What are the symptoms of Serotonin Syndrome I should look for on an exam?
On an exam, look for the classic triad of mental status changes, autonomic hyperactivity, and neuromuscular abnormalities such as spontaneous clonus or hyperreflexia. Common clinical vignettes describe patients presenting with agitation, tachycardia, diaphoresis, and “wet” skin following the addition of a second serotonergic agent. Recognizing these symptoms quickly is vital for answering high-yield questions on the NAPLEX or NCLEX and ensuring patient safety during clinical rotations.
Why does grapefruit juice interact with so many different medications?
Grapefruit juice interacts with many medications because it contains furanocoumarins that irreversibly inhibit the CYP3A4 enzyme specifically within the intestinal wall. This inhibition prevents the first-pass metabolism of various drugs, leading to significantly higher systemic concentrations than intended. Since CYP3A4 is responsible for processing about 50% of all drugs, even a single glass of juice can cause a persistent effect that lasts for several days until the body synthesizes new enzymes.
Can two drugs have a ‘beneficial’ interaction?
Yes, many drug interactions are clinically intentional and provide a synergistic or additive therapeutic advantage for the patient. A common example is the combination of an ACE inhibitor with a thiazide diuretic to manage hypertension through different physiological pathways while balancing potassium levels. Another instance is “ritonavir boosting” in HIV therapy, where a low dose of ritonavir is used to inhibit the metabolism of other protease inhibitors, maintaining higher and more effective drug concentrations.
What is the best way to memorize the CYP450 system for the NAPLEX?
The most effective way to master the CYP450 system is to move beyond simple mnemonics and focus on the most common substrates for the 3A4, 2D6, and 2C9 isoenzymes. Using a common drug interactions study guide that incorporates active recall through practice vignettes helps you visualize how these enzymes function in real-world scenarios. This method ensures you can predict interactions for new or unfamiliar drugs based on their class and primary metabolic route rather than relying on rote memorization.
How do NSAIDs affect the kidneys and drug excretion?
NSAIDs interfere with renal drug excretion by inhibiting the synthesis of prostaglandins that normally keep the afferent arteriole dilated. This leads to vasoconstriction, reduced renal blood flow, and a decrease in the glomerular filtration rate (GFR). When the GFR drops, other medications that are primarily cleared by the kidneys, such as lithium or methotrexate, can accumulate to toxic levels. This mechanism explains why NSAIDs are frequently involved in “red flag” interactions for patients with pre-existing renal impairment.