GI Pharmacology Review for PANCE: High-Yield Guide for 2026
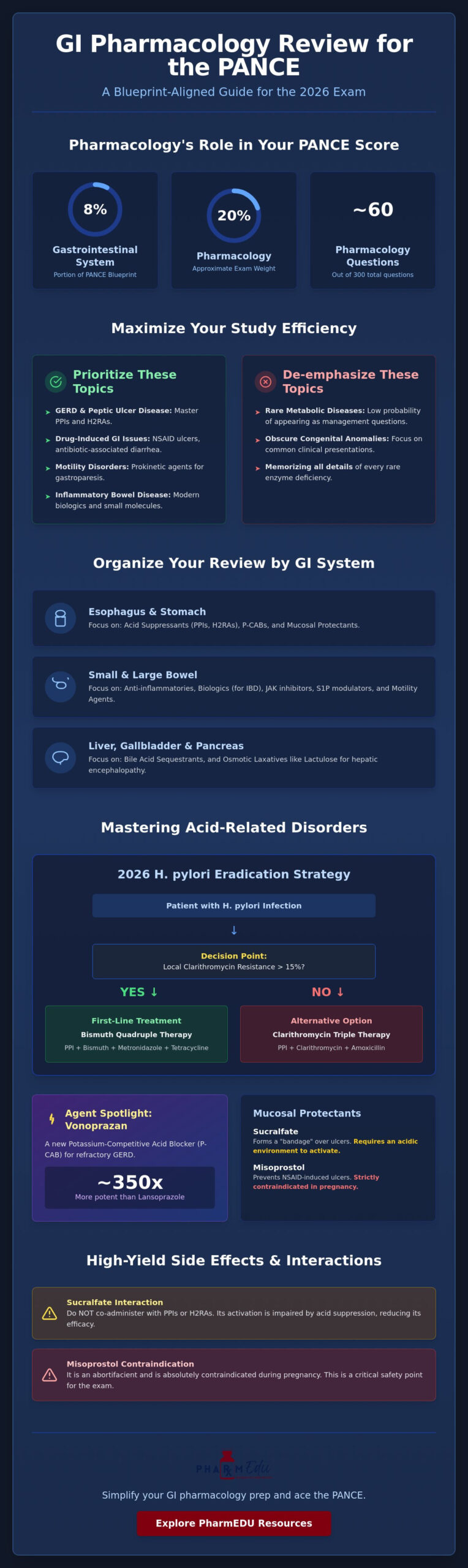
Did you know that pharmacology accounts for up to 20% of your total PANCE score? This means nearly 60 questions on your exam could hinge on your ability to select the most appropriate therapeutic agent. When you consider that the gastrointestinal system makes up 8% of the blueprint, it’s clear that a focused GI pharmacology review for PANCE is essential for your success in 2026. This isn’t just about memorizing lists; it’s about applying clinical reasoning to the latest standards of care.
We understand that the volume of information feels overwhelming. It’s difficult to distinguish between various PPIs and H2RAs, and the rapid introduction of biologics for inflammatory bowel disease only adds to the confusion. You might feel like you’re chasing a moving target as standards of care evolve. This guide simplifies that process by providing a blueprint-aligned review of high-yield drug classes and clinical pearls. You’ll master the latest 2025 AGA guidelines for Crohn’s disease and learn to identify indications for new agents like vonoprazan and etrasimod. We’ll explore the shift toward first-line biologic use and clarify the specific roles of JAK inhibitors and S1P receptor modulators, ensuring you approach the exam with the confidence of a prepared clinician.
Key Takeaways
- Understand how the NCCPA blueprint weights the gastrointestinal system to focus your study efforts on the most impactful exam topics.
- Master the clinical distinctions between PPIs and H2RAs to confidently answer management questions regarding acid-related disorders.
- Differentiate between advanced biologics and oral small molecules for IBD according to the most current 2026 therapeutic standards.
- Identify high-yield drug side effects and interactions, such as pill esophagitis, to navigate common exam traps effectively.
- Optimize your study routine by using this GI pharmacology review for PANCE alongside interactive flashcards and high-yield video vignettes.
The PANCE GI Blueprint: Why Pharmacology is Key to Your 8% Score
The NCCPA Content Blueprint for 2026 allocates 8% of the exam to the Gastrointestinal System and Nutrition. While this might seem like a manageable portion, remember that pharmacology questions comprise approximately 18-20% of the entire 300-question exam. This intersection means a significant portion of your GI questions won’t just ask for a diagnosis; they’ll require you to choose the “next best step in management,” which is almost always a pharmacological intervention. Mastering this GI pharmacology review for PANCE is about more than memorizing names; it’s about understanding why one drug is superior to another in a specific clinical scenario.
Breaking Down the 8%: What to Expect
The exam structure places a heavy emphasis on clinical application rather than rote memorization. You’ll encounter vignettes where the diagnosis is provided or easily identifiable, shifting the challenge to selecting the correct treatment. This includes managing biliary colic, gastric ulcers, and hepatic encephalopathy. GI pharmacology for PANCE 2026 encompasses the mechanisms, indications, and adverse profiles of medications used to treat disorders from the esophagus to the rectum, including nutritional support and accessory organ management.
High-Yield vs. Low-Yield GI Topics
Efficiency is your best friend when studying. Focus on conditions with high prevalence and clear first-line treatments. GERD and Peptic Ulcer Disease (PUD) are perennial favorites because they involve well-defined drug classes like PPIs and H2RAs. You should also prioritize drug-induced GI complications, such as NSAID-induced ulcers or antibiotic-associated diarrhea, as these test your ability to recognize clinical correlations.
In contrast, rare metabolic storage diseases or obscure congenital anomalies rarely appear as management-heavy questions. You’ll gain more points by understanding the role of prokinetic agents in gastroparesis than by memorizing every detail of a rare enzyme deficiency. To organize your study, categorize medications by the organ system they target:
- Esophagus and Stomach: Acid suppressants and mucosal protectants.
- Small and Large Bowel: Anti-inflammatories, biologics, and motility agents.
- Liver and Gallbladder: Bile acid sequestrants and osmotic laxatives like lactulose.
Focusing on medications with clear first-line indications in the blueprint will help you eliminate distractors quickly during the five-hour exam. By prioritizing these high-yield classes, you ensure your preparation aligns with the clinical reasoning standards expected of a practicing physician assistant.
Acid Management: Comparing PPIs, H2RAs, and Mucosal Protectants
Acid-related disorders are a cornerstone of any GI pharmacology review for PANCE. You must be able to differentiate between neutralizing existing gastric acid and preventing its secretion at the cellular level. While antacids provide rapid, transient relief by neutralizing HCl, sustained management of GERD and Peptic Ulcer Disease (PUD) requires H2-receptor antagonists (H2RAs) or Proton Pump Inhibitors (PPIs).
For H. pylori eradication, the 2026 standards emphasize bismuth-based quadruple therapy as a primary choice, particularly in regions where clarithromycin resistance exceeds 15%. This regimen typically includes a PPI, Bismuth, Metronidazole, and Tetracycline. Standard triple therapy, consisting of a PPI, Clarithromycin, and Amoxicillin, remains a viable option only if local resistance is low. A significant 2026 clinical pearl is the emergence of Vonoprazan, a potassium-competitive acid blocker (P-CAB). It’s approximately 350 times more potent than lansoprazole and provides faster, more consistent acid suppression for refractory GERD.
Mucosal protectants offer a different strategy by fortifying the stomach lining. Sucralfate creates a physical “bandage” over ulcers but requires an acidic environment to activate; therefore, you should not co-administer it with potent acid suppressants. Misoprostol, a PGE1 analog, is highly specific for preventing NSAID-induced ulcers. However, its use is limited by significant GI side effects and a strict contraindication in pregnancy due to its abortifacient properties.
Proton Pump Inhibitors (PPIs) Deep Dive
PPIs like Omeprazole and Pantoprazole are the most effective agents for acid suppression because they irreversibly inhibit the H+/K+ ATPase pump. Timing is everything for these medications. Patients must take them 30 to 60 minutes before their first meal to ensure the drug is present when the parietal cell pumps are most active. Long-term use carries specific board-relevant risks. You must monitor for B12 deficiency, as gastric acid is required to cleave B12 from dietary protein. Other risks include increased fracture rates due to impaired calcium absorption and a higher incidence of C. difficile infections.
H2RAs and Antacids
H2RAs like Famotidine are excellent for milder GERD or “on-demand” relief. Cimetidine is the classic “trap” drug for PANCE questions. It’s a potent CYP450 inhibitor and possesses anti-androgenic effects, which can lead to gynecomastia and impotence in male patients. While acid management focuses on the upper GI tract, systemic inflammatory conditions like Crohn’s or Ulcerative Colitis often require Biologic Therapies for IBD to achieve true mucosal healing. If you find these drug-drug interactions and regimens difficult to keep straight, our Interactive Pharmacology Flashcards can help you solidify these distinctions through active recall.
Advanced GI Therapeutics: Biologics for IBD and Motility Agents
Managing Inflammatory Bowel Disease (IBD) and motility disorders requires a shift from simple acid neutralization to complex immunomodulation and neuroreceptor targeting. As you refine your GI pharmacology review for PANCE, it’s vital to recognize that treatment paradigms have evolved. For example, the American Gastroenterological Association (AGA) issued updated guidelines in November 2025 that now recommend advanced biologic drugs as first-line therapy for moderate-to-severe Crohn’s disease. This “top-down” approach replaces the traditional “step-up” method, reflecting a commitment to preventing bowel damage through early, aggressive intervention.
Managing Inflammatory Bowel Disease (IBD)
Pharmacotherapy for IBD is often divided by the specific condition: Ulcerative Colitis (UC) or Crohn’s Disease. 5-Aminosalicylates (5-ASA) like Mesalamine and Sulfasalazine remain foundational for inducing and maintaining remission in UC. If a board question features Sulfasalazine, remember its unique side effect profile; it can cause folate deficiency, necessitating supplementation. For acute flares, steroids provide rapid relief. Budesonide is a high-yield favorite because its high first-pass metabolism limits systemic side effects, making it ideal for ileal or right-sided colonic Crohn’s. In contrast, Prednisone is reserved for more severe systemic presentations despite its broader side effect profile.
For refractory cases or moderate-to-severe disease, biologics like Infliximab and Adalimumab (TNF-alpha inhibitors) are standard. You should also be familiar with newer agents mentioned in the 2026 blueprint, such as the oral S1P receptor modulator Etrasimod, approved for UC, and anti-IL-23 agents like Risankizumab for Crohn’s. Immunomodulators like Azathioprine require monitoring for leukopenia and hepatotoxicity, while Methotrexate remains a secondary option for maintaining remission in Crohn’s patients who are steroid-dependent.
Antiemetics and Prokinetics
Selecting the right antiemetic depends heavily on the clinical trigger. Serotonin (5-HT3) antagonists like Ondansetron are the gold standard for chemotherapy-induced and postoperative nausea, though you must watch for QT interval prolongation. Dopamine antagonists like Promethazine offer alternative pathways but carry a higher risk of sedation and extrapyramidal symptoms.
When the issue is gastric emptying rather than simple nausea, prokinetics are required. Metoclopramide acts as a D2 antagonist, increasing lower esophageal sphincter tone and stimulating antral contractions. However, the PANCE often tests the “Black Box” warning for Metoclopramide: the risk of irreversible Tardive Dyskinesia with long-term use. For patients with gastroparesis who cannot tolerate dopamine antagonists, Erythromycin serves as a motilin receptor agonist to jump-start GI motility. Understanding these receptor-level differences allows you to choose the “next best step” with precision during the exam.
Avoiding Common Traps: High-Yield GI Drug Side Effects and Interactions
A successful GI pharmacology review for PANCE requires a deep understanding of why certain drugs are contraindicated in specific scenarios. One frequent board favorite is pill esophagitis. Medications like bisphosphonates (alendronate) and tetracyclines (doxycycline) cause direct mucosal irritation if they remain in contact with the esophageal lining. Patients must take these with a full glass of water and remain upright for at least 30 minutes. Failing to follow these instructions can lead to severe ulceration, a detail often included in clinical vignettes to test your knowledge of patient education and drug safety.
Laxatives and Antidiarrheals
You must distinguish between osmotic agents like Miralax (polyethylene glycol) and Lactulose. While both draw water into the colon, Lactulose has a specific indication for hepatic encephalopathy. It acidifies the colonic contents to trap ammonia as ammonium, facilitating its excretion. For general constipation, bulk-forming laxatives like psyllium are the safest for long-term use, whereas stimulants like senna or bisacodyl are reserved for acute relief due to the risk of dependency. In patients with opioid-induced constipation, traditional laxatives often fail. In these cases, peripherally acting mu-opioid receptor antagonists like Methylnaltrexone are the correct choice because they don’t cross the blood-brain barrier or reverse systemic analgesia.
For antidiarrheals, Bismuth subsalicylate is high-yield because it can turn stools and the tongue black, which might be mistaken for melena. Because it’s a salicylate, it carries a risk of Reye’s syndrome in children with viral illnesses. Antidiarrheals like loperamide are strictly contraindicated in cases of suspected inflammatory or infectious diarrhea, such as C. difficile or ulcerative colitis flares. Slowing down motility in these patients can lead to toxic megacolon, a life-threatening complication that examiners expect you to recognize and avoid.
Nutrition and Vitamin Pharmacology
Fat-soluble vitamin deficiencies (A, D, E, K) are common in malabsorptive states like celiac disease or chronic pancreatitis. Vitamin K deficiency is particularly critical for the PANCE because it leads to an elevated PT/INR and potential coagulopathy. When treating a patient with suspected Wernicke’s encephalopathy, you must always administer thiamine before glucose. Giving glucose first can deplete remaining thiamine stores and worsen the neurological damage. The pharmacological management of acute pancreatitis primarily involves aggressive intravenous fluid resuscitation and parenteral analgesia; no specific drug therapy currently exists to directly halt the inflammatory process.
Patients with cirrhosis require significant medication adjustments. You should avoid NSAIDs due to the risk of hepatorenal syndrome and GI bleeding. Many drugs metabolized by the liver, including certain sedatives and even acetaminophen, require dose reductions or complete avoidance. To test your ability to spot these clinical traps under exam conditions, we recommend taking our Pharmacology Practice Quizzes.
Streamlining Your Prep: How PharmEDU Simplifies GI Pharmacology
Mastering the 8% GI section of your exam requires a study tool that evolves as quickly as the clinical guidelines themselves. PharmEDU provides a GI pharmacology review for PANCE that prioritizes high-yield clinical reasoning over static drug lists. Our High-Yield Video Vignettes break down complex scenarios, such as differentiating between a routine GERD presentation and refractory cases requiring the latest P-CAB therapies. These visual aids are specifically designed to help you internalize the “next best step” logic that the 2026 NCCPA blueprint demands, making abstract mechanisms feel like concrete clinical decisions.
Why Digital Review Beats Traditional Textbooks
When comparing a comprehensive pharmacy review platform to traditional, heavy textbooks, the difference in efficiency is stark. Textbooks often lag behind the latest FDA approvals and major guideline shifts, such as the November 2025 AGA update for Crohn’s disease management. PharmEDU provides real-time updates, ensuring you aren’t studying outdated protocols when the boards expect you to know current first-line biologic initiation strategies.
The benefit of micro-learning is particularly valuable for busy PA students. Our mobile-compliant study tools allow you to engage in active recall during 15-minute breaks on clinical rotations. Whether you are using our Interactive Pharmacology Flashcards to memorize IBD biologic mechanisms or reviewing laxative classifications between patient rounds, you are consistently building the neural pathways required for long-term retention. This digital approach respects your time and reflects the modern reality of medical education.
Start Your PANCE Success Journey
Our Pharmacology Practice Quizzes mirror the actual PANCE environment, featuring vignettes that test your ability to avoid common traps like pill esophagitis or drug-induced toxic megacolon. These management-style questions are essential because simply knowing a drug name is insufficient for the 2026 exam; you must know the “why” behind every therapeutic choice. By connecting pharmacology concepts directly to clinical practice, we help you bridge the gap between classroom knowledge and professional competence.
PharmEDU supports both individual learners and those using an Institutional Platform License, providing a structured and predictable path to certification. Your journey to becoming a certified physician assistant is demanding, but you don’t have to navigate the shifting scientific landscape alone. Start your preparation today with a PharmEDU Monthly Subscription and gain the clinical edge required to master the gastrointestinal section of the 2026 PANCE with absolute confidence.
Secure Your PANCE Success with Targeted GI Prep
Mastering the GI section requires more than rote memorization; it demands a deep understanding of clinical management and the ability to navigate complex drug interactions. By focusing on high-yield drug classes and staying current with the 2025 AGA guidelines for IBD, you can confidently handle the pharmacological questions that make up a significant portion of your score. This GI pharmacology review for PANCE provides the structural framework you need to categorize treatments from acid suppression to advanced immunomodulation.
To ensure you’re fully prepared for board day, leverage tools that simplify the most challenging concepts. Our platform features high-yield video vignettes for 100+ topics, NCCPA blueprint-aligned practice quizzes, and mobile-ready interactive flashcards designed for the busy student. Master GI Pharmacology with a PharmEDU Subscription and take a definitive step toward your certification. You’ve worked hard to reach this point, and we’re here to help you cross the finish line with precision and confidence.
Frequently Asked Questions
What is the first-line treatment for H. pylori infection in 2026?
Bismuth-based quadruple therapy is the preferred first-line treatment for H. pylori in 2026, especially in areas where clarithromycin resistance is high. This regimen includes a proton pump inhibitor (PPI), bismuth subsalicylate, metronidazole, and tetracycline taken for 14 days. While triple therapy was once standard, clinicians now favor the quadruple approach to ensure higher eradication rates and overcome antibiotic resistance.
How do PPIs and H2RAs differ in their mechanism of action for the PANCE?
PPIs irreversibly inhibit the H+/K+ ATPase pump in the parietal cell, which is the final step of acid secretion. In contrast, H2RAs competitively block histamine-2 receptors on the parietal cell, reducing but not completely stopping acid production. For your GI pharmacology review for PANCE, remember that PPIs are more potent and require activation by a meal, whereas H2RAs provide faster relief for mild symptoms.
Which GI medications are contraindicated in patients with a suspected bowel obstruction?
Stimulant laxatives and prokinetic agents, such as metoclopramide, are strictly contraindicated if you suspect a mechanical bowel obstruction. Increasing peristalsis against a physical blockage significantly raises the risk of bowel perforation or severe ischemic injury. Clinical vignettes often present a patient with abdominal distention and high-pitched bowel sounds; in these cases, you should avoid any medication that forces gastrointestinal motility.
What are the high-yield side effects of Cimetidine that often appear on boards?
Cimetidine is a frequent board topic because of its significant side effect profile and drug-drug interactions. It possesses anti-androgenic properties that can lead to gynecomastia and impotence in male patients. It also acts as a potent inhibitor of the cytochrome P450 system, which can dangerously increase the serum levels of medications like warfarin, phenytoin, and theophylline.
How does the treatment of Crohn’s disease differ from Ulcerative Colitis in terms of pharmacology?
Treatment for Ulcerative Colitis (UC) relies heavily on 5-aminosalicylates (5-ASA) like mesalamine for both induction and maintenance of remission. Crohn’s disease management often bypasses 5-ASAs because they are less effective for transmural inflammation. Instead, Crohn’s treatment focuses on early use of biologics, such as TNF-alpha inhibitors or anti-IL-23 agents, to prevent complications like fistulas or strictures that aren’t typically seen in UC.
What is the ‘Step-Up’ vs ‘Top-Down’ approach in IBD management?
The ‘Step-Up’ approach starts with milder anti-inflammatory drugs and escalates to biologics only if those fail. The ‘Top-Down’ approach, which is now the 2026 standard for moderate-to-severe Crohn’s, initiates highly effective biologic therapy immediately. This shift aims to induce deep mucosal healing early in the disease course, reducing the long-term need for corticosteroids and decreasing the likelihood of future surgical interventions.
Which vitamins are most affected by chronic PPI use or malabsorption syndromes?
Chronic PPI use most commonly affects the absorption of Vitamin B12, calcium, and magnesium because these nutrients require an acidic environment for optimal uptake. In malabsorption syndromes like celiac disease, the fat-soluble vitamins (A, D, E, and K) are the most impacted. For a comprehensive GI pharmacology review for PANCE, remember that Vitamin K deficiency is particularly high-yield due to its direct effect on coagulation factors and the PT/INR.
Can Metoclopramide be used long-term for gastroparesis?
Metoclopramide is not recommended for long-term use and should generally be limited to a duration of less than 12 weeks. Prolonged exposure carries a high risk of developing tardive dyskinesia, a potentially irreversible movement disorder characterized by involuntary repetitive movements. If a patient requires chronic motility support, clinicians must carefully weigh this neurological risk against the benefits of improved gastric emptying.