Pharmacology of Diuretics Made Easy: The High-Yield Study Guide (2026)
What if mastering the pharmacology of diuretics wasn’t about brute-force memorization, but simply visualizing five specific checkpoints along the nephron? It’s a common struggle to feel lost between the proximal tubule and the collecting duct, especially when you’re trying to track how a new drug like Baxfendy impacts aldosterone or why the 2025 AHA guidelines changed the management of hypertension. We understand that confusing electrolyte shifts or mixing up loop diuretics with potassium-sparing agents can shake your confidence during high-stakes exams. This guide is designed to make the pharmacology of diuretics made easy by focusing on the logic behind the mechanism rather than just a list of names.
You’ll gain a clear, structured understanding of all five diuretic classes and learn how to predict side effects based on where they act in the kidney. We’ve updated this 2026 edition to include the latest clinical breakthroughs, from the subcutaneous Lasix ONYU to the first nasal spray diuretic, Enbumyst. This article provides a comprehensive preview of the high-yield concepts found in our pharmacology practice quizzes and interactive flashcards. By the end, you’ll have the clinical pearls and professional insights needed to tackle any board question with precision and authority.
Key Takeaways
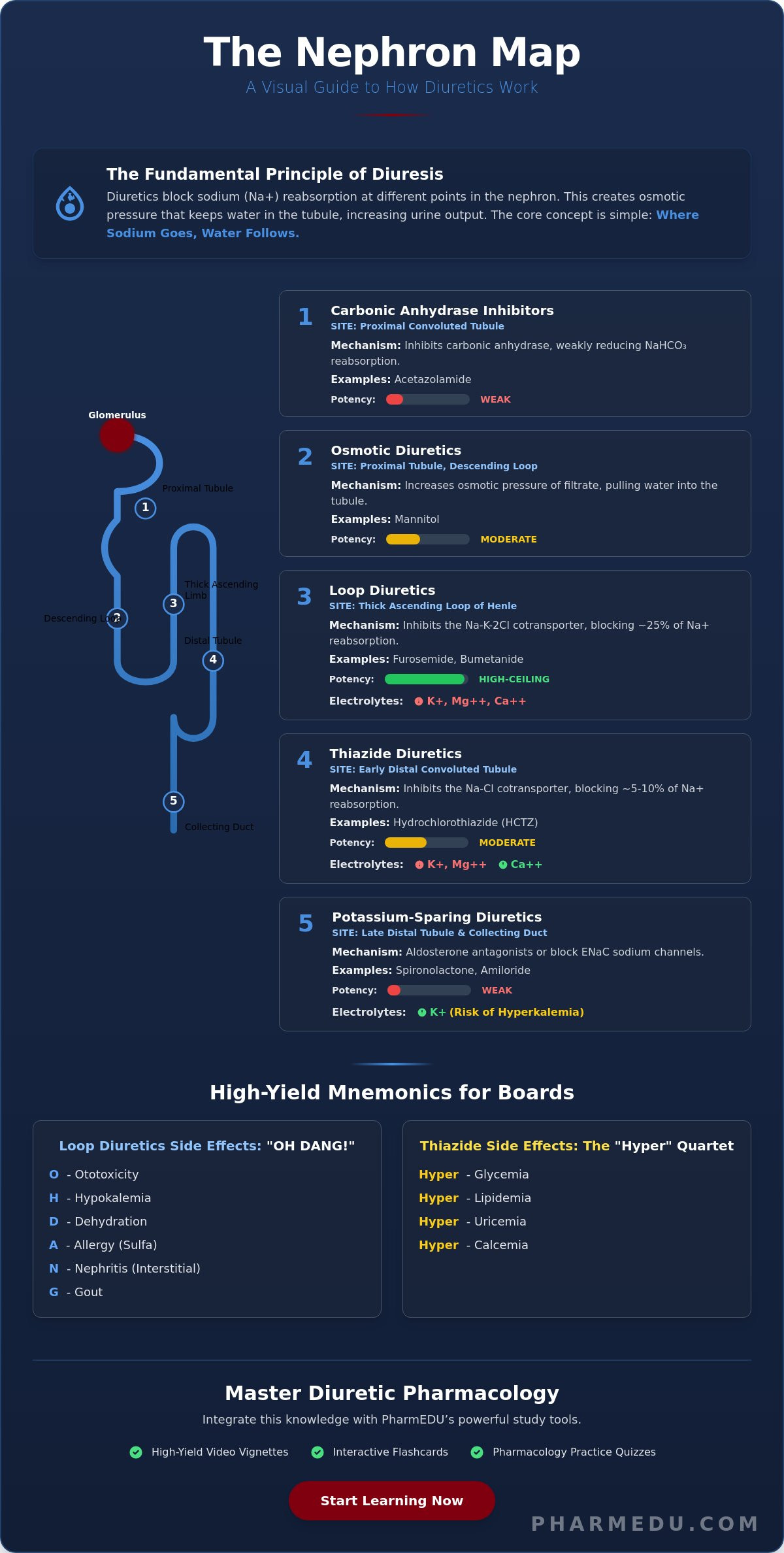
- Understand the fundamental “where sodium goes, water follows” principle to predict how different agents alter urine volume and concentration.
- Visualize the nephron spatially to make the pharmacology of diuretics made easy, linking each of the five drug classes to its specific site of action from the proximal tubule to the collecting duct.
- Compare the therapeutic potency of “high-ceiling” loop diuretics against long-acting thiazides to determine the most appropriate clinical application for each patient scenario.
- Master high-yield mnemonics like “OH DANG!” and the “Hyper” quartet to effortlessly recall complex side effect profiles and electrolyte imbalances for board exams.
- Strengthen your retention of renal mechanisms by integrating PharmEDU’s high-yield video vignettes and interactive pharmacology flashcards into your study routine.
Understanding Diuretics: The Fundamentals of Renal Pharmacology
Diuretics are essential pharmacological agents designed to increase the rate of urine flow and sodium excretion. By inhibiting the reabsorption of sodium at various segments of the renal tubule, these drugs effectively reduce extracellular fluid volume. This Diuretic overview highlights that their primary function is to manage conditions where the body retains too much fluid. While some simplified resources suggest these drugs simply “increase urination,” the clinical reality involves a complex interplay of solute transport and osmotic gradients. Mastering the pharmacology of diuretics made easy starts with grasping this fundamental mechanism: diuretics don’t move water directly; they move salt, and water simply follows.
This “Where Sodium Goes, Water Follows” principle is the cornerstone of renal physiology. When a drug blocks a sodium transporter in the kidney, the sodium remains in the tubular lumen. This creates an osmotic pressure that keeps water within the tubule, eventually leading to its excretion. This process is vital for treating hypertension, managing congestive heart failure, and reducing the peripheral edema associated with hepatic or renal dysfunction. Because these drugs are foundational to cardiovascular and renal care, they remain a high-yield focus for the USMLE, NAPLEX, and NCLEX exams. Students who use our High-Yield Video Vignettes often find that visualizing these fluid shifts is the quickest way to move beyond rote memorization.
The Role of the Nephron in Fluid Balance
The nephron acts as the functional unit of the kidney, processing approximately 180 liters of filtrate daily. This process involves three distinct stages: filtration at the glomerulus, reabsorption of essential solutes back into the blood, and secretion of waste products into the tubule. Diuretics intervene during the reabsorption phase by specifically targeting transport proteins. The nephron serves as the primary target for all diuretic therapy. Understanding exactly where each drug class acts on this microscopic structure allows you to predict clinical outcomes with precision. Our Pharmacology Practice Quizzes frequently test this spatial relationship, as it’s the key to differentiating between the five major classes.
Key Electrolytes to Monitor
Effective management requires constant vigilance over electrolyte shifts. Sodium (Na+) is the main driver of fluid movement, but it’s rarely the electrolyte that causes the most concern for clinicians. Potassium (K+) is the most critical electrolyte for diuretic-related safety; imbalances here can lead to life-threatening arrhythmias. While sodium and potassium take center stage, secondary shifts in Calcium and Magnesium are equally vital for board exams. Loop diuretics typically decrease calcium levels, whereas thiazides tend to increase them. Keeping these details straight is the reason why the pharmacology of diuretics made easy approach relies on mapping these changes to specific transporters. You can practice these distinctions using our Interactive Pharmacology Flashcards to ensure you’re ready for any clinical scenario.
Mapping the Nephron: Where Each Diuretic Class Works
Visualizing the nephron from the glomerulus to the collecting duct is the most effective way to organize your study of renal drugs. Think of the nephron as a series of specialized gates, each responsible for moving specific ions back into the bloodstream. The pharmacology of diuretics made easy approach requires you to think of this structure as a map. By identifying exactly where a drug blocks a “gate,” you can predict how much water will stay in the tubule and which electrolytes will be lost in the process. This spatial logic is far more reliable than memorizing isolated drug facts, as it allows you to deduce clinical outcomes based on renal anatomy.
The Proximal and Ascending Targets
Carbonic anhydrase inhibitors, such as acetazolamide, target the proximal convoluted tubule (PCT). While the PCT reabsorbs the bulk of filtered sodium, these drugs are relatively weak diuretics because the distal segments of the nephron can compensate for the increased sodium load. Instead, they’re used for niche clinical purposes like treating glaucoma or preventing high-altitude sickness. In contrast, loop diuretics like furosemide and bumetanide act on the thick ascending limb of the loop of Henle. The Na-K-2Cl symporter, located in the thick ascending limb of the loop of Henle, is the primary target for loop diuretics, which inhibit the simultaneous reabsorption of one sodium, one potassium, and two chloride ions. Because this segment reabsorbs about 25% of filtered sodium, loop diuretics are the most potent agents available, often referred to as “high-ceiling” diuretics.
Distal and Collecting Duct Targets
Thiazide diuretics work further down the line in the distal convoluted tubule (DCT). They inhibit the Na-Cl cotransporter, blocking the reabsorption of approximately 5% of filtered sodium. While less potent than loop agents, they’re highly effective for long-term hypertension management. Finally, potassium-sparing diuretics act in the collecting duct. This class is divided into aldosterone antagonists, like spironolactone, and sodium channel blockers, like amiloride. These agents are significantly less potent than loop diuretics because only about 1% to 2% of filtered sodium reaches the collecting duct. However, their ability to prevent potassium loss makes them invaluable in combination therapy.
Understanding the Cardiovascular effects of diuretics is crucial, as their impact on blood volume directly influences cardiac output and systemic vascular resistance. If you’re struggling to visualize these pathways during your review, our Interactive Pharmacology Flashcards offer a structured way to reinforce these site-specific mechanisms. By the time you reach the collecting duct in your study, the relationship between site of action and diuretic potency becomes clear: the earlier a drug acts in the nephron, the more sodium it can potentially block from reabsorption.
Comparing the 5 Major Classes of Diuretics
Differentiating between the various classes requires a focus on their individual high-yield characteristics. While loop diuretics are known as “high-ceiling” agents because they produce a dose-dependent increase in diuresis, thiazides reach a plateau where higher doses don’t yield more effect. This distinction makes the pharmacology of diuretics made easy for students who prioritize clinical application over raw data. Beyond potency, the duration of action varies significantly; loops are generally short-acting, whereas thiazides like chlorthalidone provide extended coverage, making them the preferred choice for chronic hypertension management. In fact, thiazides are projected to hold 39.2% of the global diuretic market share in 2026, largely due to their foundational role in blood pressure control.
A detailed review of the Therapeutic Uses of Diuretic Agents confirms that clinicians must also weigh metabolic consequences. Both loops and thiazides can lead to hyperglycemia, hyperlipidemia, and hyperuricemia, which may trigger gout flares. Drug-drug interactions are another critical area for exam preparation. NSAIDs can blunt the effectiveness of diuretics by inhibiting vasodilatory prostaglandins. Additionally, thiazides reduce the renal clearance of lithium, potentially leading to toxicity, while the hypokalemia caused by loops and thiazides significantly increases the risk of digoxin toxicity.
Loop vs. Thiazide Diuretics
The most common board exam distractor involves calcium levels. Loop diuretics “lose” calcium, leading to hypocalcemia, whereas thiazides “thirst” for it, causing hypercalcemia. This makes thiazides a strategic choice for patients with both hypertension and osteoporosis. Clinically, loops are the gold standard for acute heart failure and pulmonary edema because they provide rapid volume depletion. It’s also vital to remember that most agents in both classes are sulfonamide derivatives. Patients with severe sulfa allergies may require ethacrynic acid, the only loop diuretic without a sulfonamide component. Our Clinical Case Studies provide excellent practice for navigating these patient-specific contraindications.
Potassium-Sparing and Osmotic Agents
Potassium-sparing diuretics act in the collecting duct and are often used to counteract the potassium-wasting effects of other diuretics. Spironolactone, an aldosterone antagonist, plays a unique role in heart failure by preventing cardiac remodeling and fibrosis. In contrast, agents like triamterene and amiloride block the epithelial sodium channels (ENaC) directly. Mannitol stands alone as an osmotic diuretic. It isn’t used for hypertension; instead, it pulls water into the vascular space to treat increased intracranial pressure or acute glaucoma. If these distinctions still feel overwhelming, our High-Yield Video Vignettes break down these “exception” drugs into easy-to-digest visual lessons.
Clinical Mnemonics and Side Effects Made Easy
Mastering the pharmacology of diuretics made easy involves more than just knowing where they work; you must also anticipate how they’ll affect your patient’s physiology. High-yield exams frequently test your ability to link a drug’s mechanism to its adverse profile. For loop diuretics, the “OH DANG!” mnemonic remains the gold standard for rapid recall. It stands for Ototoxicity, Hypokalemia, Dehydration, Allergy (specifically sulfa), Nephritis (interstitial), and Gout. These side effects are a direct result of the aggressive sodium and fluid loss occurring in the thick ascending limb. Ototoxicity is a particularly critical “pearl” to remember, as it’s often associated with rapid intravenous administration of high-dose furosemide.
Thiazide diuretics present a different set of challenges, often summarized as the “Hyper” quartet. While loop diuretics cause the body to lose calcium, thiazides cause the body to retain it. This leads to the classic four: Hyperglycemia, Hyperlipidemia, Hyperuricemia, and Hypercalcemia. Potassium-sparing diuretics, particularly spironolactone, introduce unique endocrine concerns. Because spironolactone is structurally similar to steroid hormones, it can cause gynecomastia and menstrual irregularities. However, the most life-threatening concern for this class is hyperkalemia, especially when these agents are combined with ACE inhibitors or ARBs. Test your ability to recognize these side effects in real-world scenarios with our Clinical Case Studies.
Electrolyte Imbalances: The Easy Way to Remember
A simple rule of thumb will save you hours of confusion: every diuretic class except the potassium-sparing agents causes hypokalemia. This occurs because the increased sodium load reaching the distal tubule forces the body to exchange sodium for potassium, wasting the latter in the urine. This shift is dangerous for patients on heart failure medications. Low serum potassium levels increase the risk of Digoxin toxicity because potassium and Digoxin compete for the same binding site on the Na+/K+-ATPase pump, meaning less potassium results in more drug binding. Monitoring for signs of toxicity, such as yellow-green halos in the patient’s vision or bradycardia, is a mandatory clinical competency.
Nursing and Pharmacy Monitoring Pearls
Clinical management requires vigilant monitoring of vital signs and laboratory values. Assessing for orthostatic hypotension is essential, as the rapid volume depletion can lead to falls, particularly in the elderly. You must also track BUN, Creatinine, and GFR to ensure the diuresis isn’t so aggressive that it triggers an acute kidney injury. Patient education should focus on the timing of doses; patients should take their medication in the morning to avoid nocturia and sleep disruption. Furthermore, teach patients to perform daily weights and report any gain of more than two pounds in a single day. Dietary counseling is the final piece of the puzzle. Patients on “wasting” diuretics need high-potassium foods like bananas and spinach, while those on spironolactone must avoid potassium-rich salt substitutes to prevent dangerous elevations.
Mastering Diuretic Pharmacology with PharmEDU
Mastering the pharmacology of diuretics made easy requires more than just reading a guide; it demands active engagement with the material. Our platform is designed to bridge the gap between complex renal physiology and clinical confidence. PharmEDU’s High-Yield Video Vignettes break down the most challenging concepts into digestible segments, allowing you to visualize sodium transport and fluid shifts in real time. Instead of struggling with dry text, you can watch how a loop diuretic interacts with the thick ascending limb, making the underlying logic intuitive rather than burdensome. These visual tools are specifically engineered to help you retain information longer and recall it faster during high-pressure exams.
Retention is further solidified through our Interactive Pharmacology Flashcards. These aren’t simple vocabulary cards; they’re designed to cement diuretic sites of action and electrolyte patterns through spaced repetition. When you combine these with our Pharmacology Practice Quizzes, you’re not just memorizing facts. You’re training your brain to recognize the “distractor” answers that board exams frequently use. Our questions mimic the style and rigor of the NAPLEX and USMLE, ensuring that nothing on test day feels unfamiliar. To round out your preparation, our Clinical Case Studies challenge you to apply diuretic theory to real-world scenarios, such as managing a patient with both heart failure and a sulfa allergy.
Why Students Choose PharmEDU for Board Prep
Modern medical and pharmacy education is fast-paced, often leaving students with little time for traditional study methods. PharmEDU focuses on micro-learning segments that fit perfectly into the gaps of a busy clinical rotation. Whether you have five minutes between patient rounds or an hour in the library, our mobile-friendly interface ensures you can always make progress. Our evidence-based content is strictly updated for 2026 standards, incorporating the latest FDA approvals and clinical guidelines. For those just beginning their journey, we also offer a specialized pharmacology study guide for nursing students to build a strong foundational knowledge of renal agents.
Start Your Pharmacology Success Journey
The transition from feeling confused to becoming board-ready happens through structured, logical learning. We’ve seen thousands of students move past the frustration of mixing up electrolyte imbalances by using our step-by-step framework. By joining our community, you gain immediate access to a comprehensive library covering over 100 high-yield topics beyond just diuretics. Our goal is to take the administrative and mental burden of exam prep off your shoulders, allowing you to focus on becoming a prepared and capable clinician. Don’t leave your exam scores to chance. Join PharmEDU today to master pharmacology for your exams!
Take Command of Your Renal Pharmacology Prep
Successfully navigating renal pharmacology requires a shift from memorizing isolated drug names to understanding the spatial logic of the nephron. You now have the tools to link specific drug classes to their sites of action, from the high-ceiling potency of loop diuretics to the potassium-sparing mechanisms of the collecting duct. This guide has demonstrated that the pharmacology of diuretics made easy is achievable when you prioritize the “where sodium goes, water follows” principle. By mastering these foundational concepts and high-yield mnemonics, you can accurately predict electrolyte shifts and metabolic side effects in any clinical or exam scenario.
To further solidify your knowledge, our platform offers a specialized suite of tools designed for the modern student. PharmEDU is trusted by top nursing and pharmacy programs for its mobile-compliant micro-learning approach and library of over 100 high-yield video vignettes. Whether you’re on a quick clinical break or in an intensive study session, our structured resources ensure you stay board-ready. Master diuretics and pass your boards with PharmEDU; Start Now! With the right framework, you’ll approach your next exam with the confidence and precision of a seasoned professional.
Frequently Asked Questions
What is the most common side effect of loop diuretics?
The most common side effects of loop diuretics include hypokalemia, dehydration, and orthostatic hypotension. These agents are extremely potent because they act on the thick ascending limb, leading to a massive loss of sodium and water. Patients often experience a rapid drop in blood pressure, which increases the risk of falls. Clinicians must monitor for these shifts to ensure patient safety and avoid acute kidney injury during aggressive diuresis.
How do potassium-sparing diuretics differ from thiazides?
Potassium-sparing diuretics differ from thiazides primarily by their effect on serum potassium levels and their site of action. While thiazides act on the distal convoluted tubule and cause potassium wasting, potassium-sparing agents work in the collecting duct to retain potassium. This distinction is a vital part of making the pharmacology of diuretics made easy for students. Combining these classes can help maintain electrolyte balance while still achieving effective fluid removal.
Why is Spironolactone often prescribed for heart failure patients?
Spironolactone is prescribed for heart failure because it acts as an aldosterone antagonist to prevent cardiac remodeling and fibrosis. Beyond its mild diuretic effect, it blocks the harmful long-term effects of aldosterone on the heart muscle. This clinical application is crucial for improving survival rates in patients with reduced ejection fraction. It’s often used in combination with other heart failure medications to provide comprehensive cardiovascular protection and volume management.
Can diuretics be taken at night?
Patients should avoid taking diuretics at night to prevent nocturia, which is the frequent need to urinate during sleep. Taking a dose late in the evening leads to sleep deprivation and increases the risk of nighttime falls, especially in elderly populations. Clinicians typically recommend taking the first dose in the morning and a second dose, if needed, no later than 4:00 PM. This schedule ensures peak drug activity occurs during waking hours.
What is the “ceiling effect” in diuretic pharmacology?
The “ceiling effect” refers to a pharmacological plateau where increasing the drug dose no longer produces a greater diuretic response. Thiazide diuretics are known for having a relatively low ceiling, meaning they reach their maximum effectiveness at lower doses. In contrast, loop diuretics are “high-ceiling” agents because their response continues to increase across a much wider dosage range. Understanding this limit helps clinicians decide when to switch classes rather than simply increasing a dose.
Which diuretic is used to treat increased intracranial pressure?
Mannitol is the primary diuretic used to treat increased intracranial pressure and cerebral edema. As an osmotic agent, it stays within the vascular space and pulls water out of the brain tissues through an osmotic gradient. This reduces pressure before permanent neurological damage occurs. Unlike other diuretics, mannitol is administered intravenously and isn’t typically used for systemic hypertension or peripheral edema management because of its unique mechanism.
How do NSAIDs interfere with the effectiveness of diuretics?
NSAIDs interfere with diuretics by inhibiting the production of vasodilatory prostaglandins in the kidneys. Prostaglandins help maintain renal blood flow and support the action of many diuretic agents. When these are blocked, the kidneys experience vasoconstriction, which reduces the delivery of the diuretic to its site of action. This interaction often leads to fluid retention and a significant decrease in the effectiveness of blood pressure management.
What electrolyte imbalance is most concerning with Furosemide?
Hypokalemia is the most concerning electrolyte imbalance associated with Furosemide therapy. Because Furosemide is a potent loop diuretic, it causes a significant amount of potassium to be excreted in the urine. Low potassium levels can trigger life-threatening cardiac arrhythmias and increase the risk of toxicity for patients taking digoxin. Mastering the pharmacology of diuretics made easy requires recognizing that frequent lab monitoring is the only way to catch these shifts early.