Anticoagulants Mechanism of Action: A High-Yield Pharmacology Guide (2026)
If you’re still memorizing andexanet alfa as the primary reversal agent for Factor Xa inhibitors, your board exam preparation is already outdated. Following its withdrawal from the U.S. market in December 2025, the clinical landscape for managing bleeding has shifted significantly. Mastering the anticoagulants mechanism of action is no longer just about memorizing a static chart; it’s about staying current with evolving standards like the 2026 ACC/AHA guidelines that now prefer DOACs for acute pulmonary embolism management.
We know that keeping the Roman numeral factors of the coagulation cascade straight can feel like an impossible task, especially when you’re also trying to differentiate between indirect and direct inhibitors. This high-yield guide simplifies these complex pathways into a board-focused breakdown of drug mechanisms. You’ll gain a clear visualization of the cascade and the confidence to distinguish between Heparins, Warfarin, and DOACs. We will explore the molecular targets of current therapies and look ahead at emerging Factor XI inhibitors to ensure you’re fully prepared for your next pharmacology assessment.
Key Takeaways
- Differentiate between anticoagulants, antiplatelets, and thrombolytics to ensure precision when answering high-yield pharmacology board questions.
- Master the anticoagulants mechanism of action by distinguishing between indirect inhibitors that require co-factors and direct-acting agents like DOACs.
- Identify the specific laboratory monitoring requirements, such as aPTT and INR, and understand why certain modern classes do not require routine testing.
- Learn the current high-yield reversal agents for each drug class to confidently manage clinical bleeding complications and toxicity scenarios.
- Strengthen your recall of the coagulation cascade using interactive flashcards and video vignettes designed for long-term professional mastery.
Understanding the Coagulation Cascade: The Foundation of Anticoagulant Action
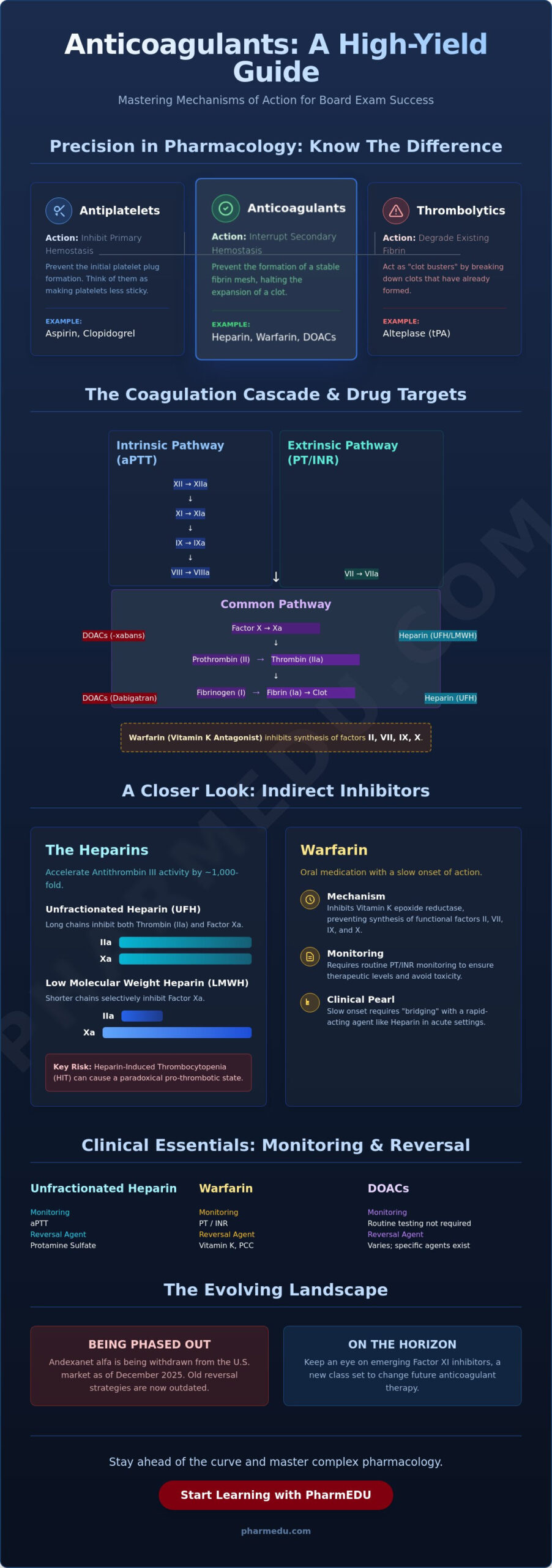
To master the anticoagulants mechanism of action, you must first visualize the complex interplay of proteins within the blood. Anticoagulants are pharmacologic agents designed specifically to interrupt the secondary hemostasis pathway. While they are often colloquially called blood thinners, they don’t actually change the viscosity of the blood. Instead, they prevent the formation of a stable fibrin mesh. It’s vital for board exams to distinguish these from other hematologic drugs. Antiplatelets, such as aspirin, inhibit primary hemostasis by preventing the initial platelet plug. Thrombolytics, like alteplase, act as clot busters by degrading existing fibrin. Anticoagulants sit in the middle; they prevent the expansion of a clot by halting the sequential activation of clotting factors.
The physiological process, often described as the coagulation cascade, functions like a waterfall. One factor activates the next in a proteolytic chain reaction. This process culminates in the common pathway, where Factors X, V, II, and I work together to produce the final structural component of a clot. Most modern therapies target this common pathway, specifically focusing on Factor Xa or Thrombin, because inhibiting these central hubs provides the most efficient control over the entire process. Understanding this foundation is the first step toward clinical proficiency and exam success.
Intrinsic vs. Extrinsic Pathways
The cascade is traditionally divided into two entry points that merge into the common pathway. The extrinsic pathway is triggered by Tissue Factor (Factor III) following vascular injury. It’s the faster, more explosive pathway and serves as the primary target for monitoring Vitamin K Antagonists like Warfarin using the Prothrombin Time (PT). In contrast, the intrinsic pathway involves contact activation of Factor XII. It’s a more complex, multi-step process that’s typically evaluated when monitoring heparin therapy through the activated Partial Thromboplastin Time (aPTT).
The Central Role of Thrombin (Factor IIa)
Thrombin, or Factor IIa, isn’t just another step in the chain. It’s the master regulator of the entire system. Its primary role is converting soluble fibrinogen into insoluble fibrin strands, which cross-link to stabilize the platelet plug. Beyond this, thrombin exerts a powerful positive feedback effect. It travels back up the cascade to activate Factors V, VIII, and XI. This action dramatically amplifies the production of more thrombin, creating an exponential growth of the clot. This feedback loop explains why the anticoagulants mechanism of action often focuses on Thrombin; if you stop the master regulator, you stop the entire amplification process.
Indirect Thrombin and Factor Xa Inhibitors: Heparin and Warfarin
Traditional anticoagulants don’t work in isolation. Instead, they function as “indirect” inhibitors, meaning they require endogenous co-factors or the interruption of metabolic cycles to exert their effects. This indirect anticoagulants mechanism of action is why certain drugs work instantly while others require days of lead time. Heparins are parenteral agents, administered either intravenously or subcutaneously, providing rapid anticoagulation. In contrast, Warfarin is an oral medication that dictates a much slower clinical pace. Understanding these molecular nuances is essential for both safe prescribing and passing rigorous pharmacology boards.
The Heparin-Antithrombin III Complex
Heparin’s efficacy depends entirely on its ability to bind to Antithrombin III (ATIII). Both Unfractionated Heparin (UFH) and Low Molecular Weight Heparin (LMWH) contain a specific pentasaccharide sequence that binds to ATIII, inducing a conformational change that accelerates its activity by 1,000-fold. The difference lies in their molecular weight and length. UFH is a long-chain polysaccharide (~15,000 Daltons) that acts as a scaffold, allowing ATIII to bind and inhibit both Thrombin (IIa) and Factor Xa. LMWH is much shorter (~5,000 Daltons). Its shorter chains are insufficient to wrap around Thrombin, making it highly selective for Factor Xa inhibition. Students often struggle with Heparin-Induced Thrombocytopenia (HIT), a type II hypersensitivity reaction where antibodies form against the Heparin-Platelet Factor 4 complex, leading to a paradoxical pro-thrombotic state. You can master these distinctions using High-Yield Video Vignettes that visualize these molecular interactions.
Warfarin and Vitamin K Epoxide Reductase
Warfarin functions by inhibiting the enzyme Vitamin K Epoxide Reductase (VKORC1). This blockage prevents the recycling of Vitamin K, which is a necessary co-factor for the gamma-carboxylation of clotting factors II, VII, IX, and X. Because Warfarin only prevents the synthesis of *new* factors, it has no effect on those already circulating in the plasma. This explains the characteristic 3-to-5-day delay in therapeutic effect. This Anticoagulation clinical guide highlights a critical exam trap: Warfarin also inhibits Protein C and S, which are natural anticoagulants. Since Protein C has a shorter half-life than the pro-coagulant factors, patients enter a transient pro-thrombotic state during the first 48 hours of therapy. Clinicians manage this using a “Warfarin bridge,” starting a fast-acting agent like Heparin simultaneously until the International Normalized Ratio (INR) reaches the therapeutic range.
The Rise of DOACs: Direct Factor Xa and Thrombin Inhibitors
Direct Oral Anticoagulants (DOACs) represent a paradigm shift in how clinicians manage thromboembolic risks. Unlike the indirect inhibitors discussed previously, these agents don’t require a co-factor like Antithrombin III to exert their effects. This anticoagulants mechanism of action involves binding directly to the active site of specific clotting factors, which results in highly predictable pharmacokinetics and pharmacodynamics. Because their effect is dose-dependent and consistent across diverse patient populations, routine laboratory monitoring of the International Normalized Ratio (INR) or activated Partial Thromboplastin Time (aPTT) is no longer a clinical necessity. The 2026 ACC/AHA guidelines for acute pulmonary embolism management now explicitly prefer DOACs over Vitamin K antagonists for most patients, reinforcing their status as the modern standard of care.
One of the most significant clinical advantages of DOACs is their rapid onset and offset. While Warfarin takes days to reach a therapeutic steady state, DOACs achieve peak plasma concentrations within two to four hours of administration. This eliminates the need for the “Heparin bridge” in many scenarios. However, this rapid offset also means that medication adherence is critical; missing even a single dose can quickly leave a patient unprotected. Clinicians must also prioritize renal function assessments, as all DOACs rely on renal clearance to varying degrees. For instance, the first generic versions of Rivaroxaban, approved in March 2025, still require careful dose adjustments based on creatinine clearance to avoid toxic accumulation. You can practice these dosing calculations and clinical scenarios using our Pharmacology Practice Quizzes to ensure you’re exam-ready.
Direct Factor Xa Inhibitors (The “-xabans”)
Agents such as Rivaroxaban, Apixaban, and Edoxaban function by binding directly to the active site of Factor Xa. This prevents the factor from interacting with the prothrombinase complex, effectively halting the production of thrombin before it even begins. By targeting this specific step in the Physiology of Coagulation Pathways, these drugs stop the common pathway at its inception. This direct inhibition is highly efficient because one molecule of Factor Xa can catalyze the generation of over 1,000 molecules of thrombin.
Direct Thrombin Inhibitors (DTIs)
Dabigatran is the primary oral representative of this class, acting as a univalent direct thrombin inhibitor. Unlike Heparin, which only inhibits free thrombin, DTIs are effective against both free and clot-bound thrombin. This makes them particularly potent in preventing the expansion of existing thrombi. In the inpatient setting, parenteral DTIs like Argatroban and Bivalirudin remain the gold standard for managing patients with Heparin-Induced Thrombocytopenia (HIT). They provide a safe alternative for anticoagulation when the use of Heparin is strictly contraindicated due to immune-mediated complications.
Monitoring and Reversal: Clinical Pharmacology and Board Essentials
Clinical safety hinges on your ability to monitor and, if necessary, neutralize the effects of these drugs. Understanding the anticoagulants mechanism of action allows you to predict which laboratory parameters will shift during therapy. When a patient presents with a supratherapeutic level, the risk of life-threatening hemorrhage increases significantly. For board exams, you must be able to match the drug to its specific monitoring profile and its corresponding reversal strategy. This knowledge is particularly critical in 2026, as several long-standing protocols for reversal agents have recently changed due to updated safety data.
Managing patients for elective surgery also requires a deep understanding of pharmacokinetics. Because DOACs have relatively short half-lives, they typically only require a 24 to 48-hour cessation period before most procedures. Warfarin, however, necessitates a much longer lead time of five days to allow for the endogenous synthesis of clotting factors. If you’re struggling to keep these timelines and antidotes straight, you can reinforce your memory using our Interactive Pharmacology Flashcards, which are specifically designed for rapid recall of Roman numeral associations and clinical pearls.
Lab Monitoring: aPTT vs. PT/INR
The activated Partial Thromboplastin Time (aPTT) is the standard for monitoring Unfractionated Heparin because it evaluates the intrinsic and common pathways. In contrast, the Prothrombin Time (PT) and the International Normalized Ratio (INR) are used for Warfarin, as they are sensitive to the Vitamin K-dependent factors in the extrinsic pathway. LMWH and DOACs generally don’t require routine monitoring because their pharmacokinetics are highly predictable. However, in cases of renal failure or extreme obesity, an Anti-Factor Xa assay may be utilized to ensure safe dosing levels.
Antidotes and Reversal Strategies
Reversal protocols are a high-yield area for any pharmacology assessment. Protamine sulfate remains the primary agent for Heparin reversal; it works by ionically binding to the acidic heparin molecule to form a stable, inactive salt. Warfarin reversal is achieved through Vitamin K for slow correction or Four-Factor Prothrombin Complex Concentrate (Kcentra) for emergency situations. For the Direct Thrombin Inhibitor Dabigatran, Idarucizumab (Praxbind) provides immediate neutralization.
A critical update for 2026 involves Factor Xa inhibitors. You should be aware that andexanet alfa (Andexxa) was withdrawn from the U.S. market on December 22, 2025. The FDA concluded that the risks of serious thromboembolic events, which occurred in 10.3% of patients in the ANNEXA-I trial, outweighed the clinical benefits. Currently, clinical management of Factor Xa inhibitor bleeding has reverted to the use of high-dose Prothrombin Complex Concentrates while new, safer reversal agents remain in development.
Mastering Complex Pharmacology with PharmEDU’s High-Yield Resources
Memorizing the coagulation cascade is just the beginning of your professional journey. The real challenge lies in applying the anticoagulants mechanism of action to high-stakes clinical scenarios where patient safety depends on your split-second decisions. PharmEDU was designed to bridge this gap by transforming dense, academic theory into actionable, high-yield knowledge. Our platform serves as a digital mentor. We help you navigate the shift from traditional indirect inhibitors to the latest DOAC protocols with clinical precision and confidence.
Why Micro-Learning Works for Pharmacology
Traditional study methods often fail because they overwhelm the brain with too much data. We solve this problem by breaking down the complex waterfall of factors into 5-minute High-Yield Video Vignettes. These targeted segments focus on a specific pathway or drug class. This makes it easier to retain molecular interactions without the burnout. Our mobile-compliant design ensures you can study effectively during clinical rotations or in the short breaks between patient rounds. If you’re looking for a broader foundation, The Ultimate Pharmacology Study Guide for nursing students in 2026 provides a structured roadmap for your academic success.
Prepare for the NAPLEX and Beyond
Whether you’re preparing for the NAPLEX, USMLE, or specialized institutional exams, PharmEDU offers the premier tools for board review. Success requires the right tools. Our Interactive Pharmacology Flashcards use spaced repetition to reinforce Roman numeral factor associations, while our Pharmacology Practice Quizzes simulate the pressure of the testing center. Through our Clinical Case Studies, you’ll practice managing supratherapeutic INRs and navigating the 2026 reversal agent updates in a risk-free, simulated environment. We also provide Institutional Platform Licenses for universities and pharmacy schools that want to provide their students with the highest standard of digital education.
Mastery of the anticoagulants mechanism of action is just one essential piece of the pharmacologic puzzle. You can explore our comprehensive library of resources, including the ACE Inhibitors Pharmacology: The High-Yield Guide for Healthcare Students (2026), to round out your cardiovascular expertise. Join our community of healthcare professionals today by choosing a PharmEDU Monthly or Annual Subscription. Let’s take the administrative and cognitive burden out of your professional development. Focus on what matters most: providing exceptional patient care.
Advance Your Expertise in Hematologic Pharmacology
We’ve navigated the foundational coagulation cascade and analyzed how different drug classes intervene at specific molecular levels. You now understand the critical distinctions between indirect inhibitors like Heparin and the direct-acting pharmacokinetics of modern DOACs. Staying updated on the anticoagulants mechanism of action is vital for patient safety, especially with the 2026 landscape shifting toward DOAC-first protocols and the significant changes in reversal agent availability. This level of precision ensures you don’t just pass your exams but also provide the highest standard of care in high-pressure clinical environments.
To solidify this knowledge, leverage our mobile-compliant micro-learning platform designed for busy professionals. With over 100 high-yield topics covered through High-Yield Video Vignettes, PharmEDU provides the structured clarity you need for board exams. You can bridge the gap between complex theory and bedside practice using our interactive quizzes and clinical case studies. Master Anticoagulants with PharmEDU High-Yield Videos and ensure you’re prepared for every pharmacologic challenge you’ll face.
Your commitment to continuous learning is the ultimate safeguard for your patients. We’re proud to be your trusted partner as you advance through your professional journey.
Frequently Asked Questions
What is the difference between direct and indirect anticoagulants?
Indirect anticoagulants require a co-factor or the interruption of a metabolic pathway to exert their effects. For example, Heparin relies on Antithrombin III, while Warfarin interferes with the Vitamin K cycle. Direct anticoagulants bind specifically to the active site of a clotting factor without needing a helper molecule. This distinction is fundamental to understanding the anticoagulants mechanism of action across different drug classes.
How does Warfarin inhibit the coagulation cascade?
Warfarin inhibits the enzyme Vitamin K Epoxide Reductase (VKORC1), which prevents the recycling of Vitamin K. Without reduced Vitamin K, the liver cannot perform gamma-carboxylation on specific clotting factors. This results in the production of biologically inactive factors that cannot bind to calcium or phospholipid surfaces. This process effectively halts the cascade at the synthesis level rather than by neutralizing active factors.
Which clotting factors are Vitamin K-dependent?
The Vitamin K-dependent clotting factors are Factors II, VII, IX, and X. Additionally, the natural anticoagulants Protein C and Protein S require Vitamin K for their synthesis. For board exams, students often use the mnemonic 1972 to remember Factors X, IX, VII, and II. Understanding these dependencies is crucial for predicting how Vitamin K antagonists will affect laboratory parameters like PT and INR. For those interested in the broader role of nutrition and health, you can learn more about E-Nutrient for a professional selection of vitamin supplements.
Why does Heparin work faster than Warfarin?
Heparin works instantly because it activates pre-existing Antithrombin III to neutralize factors already circulating in the plasma. Warfarin has a delayed onset because it only prevents the synthesis of new factors. The clinical effect of Warfarin only appears after the body has naturally depleted the pre-existing, active clotting factors, which typically takes between 72 and 120 hours.
What is the mechanism of action for Rivaroxaban and Apixaban?
Rivaroxaban and Apixaban are direct Factor Xa inhibitors that bind specifically to the active site of Factor Xa. By blocking this factor, they prevent the conversion of prothrombin to thrombin. This targeted anticoagulants mechanism of action in the common pathway provides a highly predictable therapeutic response. Because of this consistency, these agents do not require the routine laboratory monitoring associated with older therapies.
How do Direct Thrombin Inhibitors (DTIs) differ from Heparin?
DTIs bind directly to Thrombin (Factor IIa) and can inhibit both free and clot-bound thrombin. Heparin requires Antithrombin III as a scaffold and is primarily effective against free thrombin. This unique binding property makes DTIs particularly useful in conditions like Heparin-Induced Thrombocytopenia (HIT). In these cases, heparin-based products are strictly contraindicated due to the risk of immune-mediated thrombosis.
What is the reversal agent for Dabigatran?
The specific reversal agent for Dabigatran is Idarucizumab, marketed under the name Praxbind. It’s a humanized monoclonal antibody fragment that binds to Dabigatran with an affinity approximately 350 times higher than that of thrombin. This binding neutralizes the anticoagulant effect within minutes. It’s a critical tool for clinicians managing life-threatening bleeding or patients requiring emergency surgery.
Why is Factor Xa considered a superior target for anticoagulation?
Factor Xa sits at the start of the common pathway, where the intrinsic and extrinsic pathways merge. Targeting Factor Xa is highly efficient because a single molecule of Xa catalyzes the formation of approximately 1,000 molecules of thrombin. By inhibiting Xa, clinicians can achieve profound anticoagulation. This upstream intervention effectively prevents the massive amplification of thrombin that leads to stable clot formation.