Common Drug-Food Interactions to Know: A High-Yield Guide for 2026
Did you know that 61.6% of nursing home residents experienced at least one potential drug interaction in recent years? This statistic highlights a massive challenge for healthcare professionals who must balance complex regimens with everyday dietary habits. It’s natural to feel anxious about the volume of pharmacology data required for your board exams, or to worry about making a critical safety error in a busy clinical setting. You’ve likely spent hours staring at tables of contraindications, wishing for a more logical way to retain this information.
This guide empowers you to master the most common drug-food interactions to know for 2026 through a focus on predictable PK/PD mechanisms rather than just rote memorization. We’ll dive into the latest regulatory shifts, such as the FDA’s proposed mandatory GRAS notifications and the rising “Food is Medicine” movement that is reshaping chronic disease management. You’ll gain the specific insights needed to improve your pharmacology scores and provide high-quality counseling to your patients. We’ve structured this overview to be a reliable partner in your professional development, ensuring you stay ahead of evolving safety standards and clinical expectations.
Key Takeaways
- Decode the pharmacokinetic and pharmacodynamic mechanisms that govern how nutrients alter drug efficacy, moving from rote memorization to logical clinical application.
- Identify the most common drug-food interactions to know for 2026, focusing on high-yield examples like the Cytochrome P450 system’s role in grapefruit juice interactions.
- Develop standardized counseling protocols for high-risk medications to ensure patient safety and improve adherence in diverse clinical environments.
- Utilize interactive study tools and video vignettes to bridge the gap between theoretical pharmacology data and real-world clinical case management.
- Prepare for upcoming board exams by mastering the specific dietary restrictions and mechanisms frequently tested in high-stakes pharmacology sections.
Understanding the Clinical Impact of Drug-Food Interactions
Drug-food interactions represent a complex intersection where nutrition meets pharmacology. While most practitioners prioritize drug-drug interactions, the impact of a patient’s diet on their medication profile is equally critical. These interactions can either diminish a drug’s therapeutic efficacy or escalate its toxicity to dangerous levels. For instance, Grapefruit-drug interactions serve as a classic example of how a common dietary choice can inhibit intestinal enzymes, leading to toxic systemic concentrations of statins or calcium channel blockers. Understanding the common drug-food interactions to know is no longer just an academic exercise; it’s a fundamental requirement for patient safety.
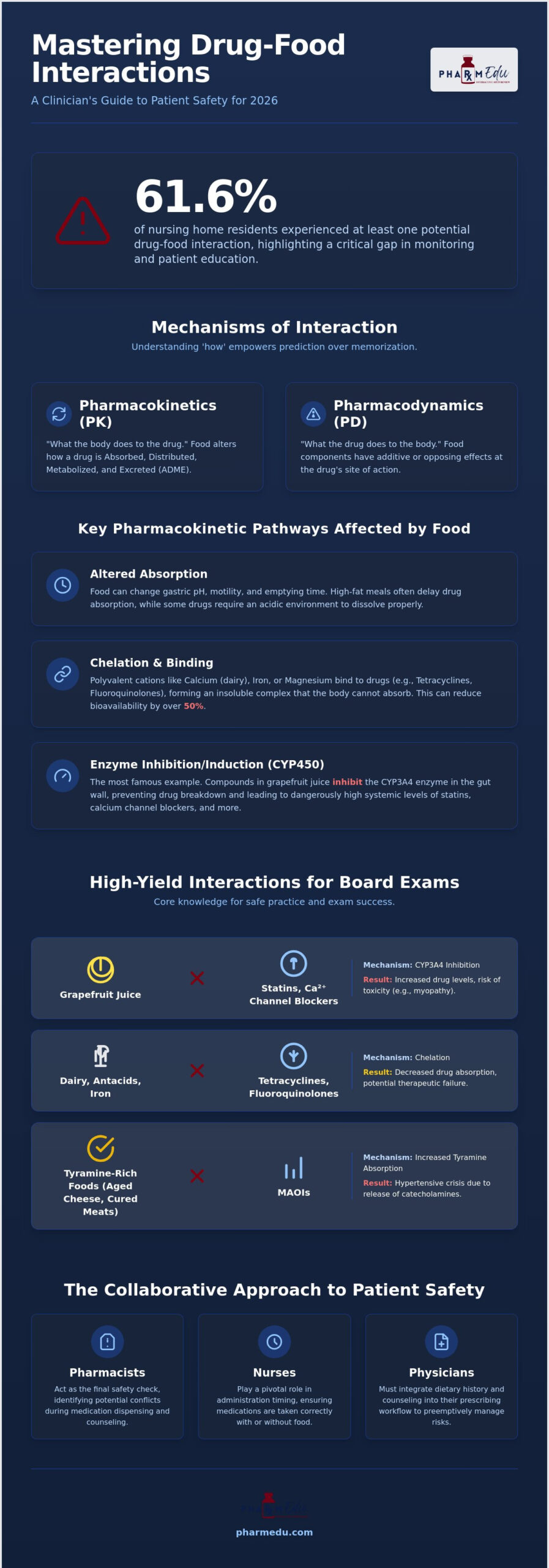
In outpatient settings, these interactions often act as a “silent threat.” Unlike clinical trials where diets are controlled, real-world patients have varied and sometimes unpredictable nutritional habits. Research spanning 2018 to 2020 found that 61.6% of nursing home residents experienced at least one potential interaction. This suggests a widespread gap in monitoring and education. With nearly 18 million U.S. households facing food insufficiency as of June 2025, the challenge isn’t just what patients eat, but also the consistency of their intake. Irregular meal patterns can lead to significant fluctuations in drug absorption and bioavailability.
The safety and economic burden of preventable adverse drug events (ADEs) is immense. As prescription drug spending is projected to grow by 10% to 12% in 2026, the clinical community must focus on every variable that influences drug response. Mastering the common drug-food interactions to know helps reduce hospital readmissions and improves the overall cost-effectiveness of pharmacological therapy.
Why Healthcare Students Must Master This Topic
Aspiring clinicians preparing for the NAPLEX, NCLEX, or USMLE will find that pharmacology sections are increasingly focused on clinical competency rather than simple drug names. 2026 standards emphasize the transition from classroom theory to bedside application. You’re expected to predict how a high-protein diet might interfere with Levodopa or why a patient on an MAOI must avoid tyramine-rich foods. These aren’t just trivia points. They’re the foundation of safe practice and high-yield exam performance.
The Role of the Clinician in Identifying Risks
Every member of the healthcare team serves as a barrier against ADEs. Pharmacists act as the final safety check, identifying potential conflicts during the medication use process. Nurses play a pivotal role in the timing of administration, ensuring medications are taken with or without food as required. Meanwhile, physicians must integrate dietary counseling into their prescribing workflow. This collaborative approach ensures that dietary restrictions don’t become a barrier to successful treatment outcomes.
Mechanisms of Interaction: Pharmacokinetics and Pharmacodynamics
Mastering the mechanics behind the common drug-food interactions to know allows clinicians to predict outcomes rather than just memorizing lists. These interactions typically occur through pharmacokinetic (PK) changes, affecting how the body handles the drug, or pharmacodynamic (PD) changes, where the food and drug have additive or opposing effects. During the absorption phase, food can significantly alter gastric pH and motility. A high-fat meal might delay gastric emptying, which slows the absorption of certain analgesics, while other medications require an acidic environment for proper solubility. If the stomach pH is raised by food or concurrent antacids, the drug may not dissolve fully, leading to therapeutic failure.
Chelation and Adsorption in the Gut
One of the most frequent absorption-based issues is chelation. This occurs when polyvalent metallic cations, such as calcium in dairy products or iron in fortified cereals, physically bind to drug molecules. This “binding” effect creates an insoluble complex that the gut cannot absorb. Tetracyclines and fluoroquinolones are particularly susceptible to this mechanism. When a patient takes a ciprofloxacin tablet with a glass of milk, the resulting chelation can reduce the drug’s bioavailability by over 50%. To prevent this, clinicians must educate patients on staggered dosing, typically recommending that the medication be taken two hours before or six hours after consuming mineral-rich foods.
The Cytochrome P450 System and Food
The metabolism phase is where the most dangerous interactions often occur, primarily involving the Cytochrome P450 (CYP) enzyme superfamily. The Cytochrome P450 enzyme system serves as the primary pathway for the oxidative biotransformation of drugs, significantly influencing their systemic concentration and therapeutic duration. CYP3A4, the most abundant enzyme in the small intestine and liver, is highly sensitive to dietary components. For example, furanocoumarins found in grapefruit juice act as potent irreversible inhibitors of intestinal CYP3A4. This inhibition prevents the first-pass metabolism of drugs like felodipine or certain statins, causing plasma levels to spike. Clinicians can refer to the FDA patient safety guide to better explain these risks to patients who regularly consume citrus juices.
Pharmacodynamic interactions are equally vital to monitor. These occur when food components directly interfere with the drug’s mechanism of action at the receptor level. A classic example is the antagonism between Vitamin K-rich leafy greens and warfarin. Because warfarin works by inhibiting the synthesis of Vitamin K-dependent clotting factors, a sudden increase in dietary Vitamin K can effectively neutralize the drug’s anticoagulant effect. Conversely, some interactions are synergistic, such as the dangerous rise in blood pressure that occurs when tyramine-rich aged cheeses are consumed alongside Monoamine Oxidase Inhibitors (MAOIs). To visualize these complex enzyme pathways and receptor interactions, many students find our High-Yield Video Vignettes to be an essential supplement to their clinical studies.
5 High-Yield Drug-Food Interactions Every Student Must Memorize
Identifying the most common drug-food interactions to know is essential for any clinician. While thousands of potential conflicts exist, these five pairs appear most frequently on standardized exams and carry the highest clinical risk. For a broader context on how these fit into general medication safety, the FDA guide to drug interactions provides a foundational perspective on managing these risks in a professional setting.
Grapefruit and the CYP3A4 Pathway
Furanocoumarins in grapefruit juice irreversibly inhibit intestinal CYP3A4 enzymes. This causes a dramatic rise in the serum levels of drugs like Simvastatin, Atorvastatin, and Felodipine. For statins, this elevation significantly increases the risk of rhabdomyolysis. Board Tip: If a clinical case study mentions a patient starting a statin and later presenting with unexplained muscle pain or dark urine, look for grapefruit consumption in their social history as the likely trigger.
Vitamin K and Warfarin Stability
Warfarin functions by inhibiting the synthesis of Vitamin K-dependent clotting factors, specifically factors II, VII, IX, and X. Leafy green vegetables like spinach and kale act as direct antagonists to this process. The clinical goal isn’t to eliminate these vegetables entirely. Instead, you must counsel patients to maintain strict dietary consistency. A sudden surge in Vitamin K intake will drop the patient’s INR, increasing the risk of thromboembolism. You can explore these mechanisms further in our resource, Pharmacology: The Comprehensive Guide to the Science of Drugs.
Tyramine and the “Cheese Effect”
Patients taking Monoamine Oxidase Inhibitors (MAOIs) must avoid aged cheeses, cured meats, and fermented products. These foods contain high levels of tyramine, which is normally broken down by MAO. When MAO is inhibited, tyramine triggers the massive release of stored norepinephrine. The “Cheese Effect” describes a life-threatening hypertensive crisis caused by the ingestion of tyramine-rich foods while taking Monoamine Oxidase Inhibitors. This results in severe occipital headaches and potential cardiovascular collapse.
Dairy, Alcohol, and Antibiotics
Chelation remains a top priority for students and practitioners. Calcium in dairy products traps Tetracyclines and Fluoroquinolones in the gut, rendering them ineffective. Additionally, the interaction between Metronidazole and alcohol is a classic test question. Metronidazole inhibits acetaldehyde dehydrogenase, leading to a Disulfiram-like reaction. Patients experience severe nausea, vomiting, and flushing if they consume even small amounts of alcohol during or shortly after treatment. Mastering these common drug-food interactions to know ensures you can catch these errors before they reach the patient.
Clinical Management and Patient Education Strategies
Effective clinical management requires moving beyond identifying risks to implementing actionable education strategies. One of the most fundamental concepts for patients is the “empty stomach” versus “with food” instruction. Generally, taking a medication on an empty stomach means one hour before or two hours after eating. This timing ensures that food doesn’t impede the solubility or absorption of the drug. Conversely, some medications require food to enhance bioavailability or to provide a buffer against gastrointestinal irritation. Developing a standardized dietary screening tool as part of Medication Therapy Management (MTM) allows you to systematically identify common drug-food interactions to know during every patient encounter. This proactive approach prevents adverse events before they compromise therapy.
Effective Patient Counseling Techniques
When educating patients, the “Teach-Back” method is an essential technique to confirm understanding. Instead of simply asking if they understand, have the patient explain in their own words how they’ll adjust their diet. Visual aids, such as high-contrast handouts, can simplify the complex science behind enzyme inhibition for non-clinical audiences. It’s also vital to address the pervasive misconception that “natural” products are inherently safe. Patients often assume that because a supplement or food is plant-based, it cannot interfere with their chemical prescriptions. In reality, these substances can be potent enzyme inducers or inhibitors that require the same scrutiny as any synthetic drug.
Staggered Dosing: A Practical Solution
Staggered dosing provides a practical solution for interactions involving chelation, such as those between dairy and certain antibiotics. A reliable rule of thumb is to administer the medication at least two hours before or four hours after consuming mineral-rich foods. However, if a patient’s diet is heavily reliant on these items, staggering may not be feasible. When staggering isn’t enough, switching to alternative therapies with different absorption profiles becomes necessary. For those in a hospital setting, The Ultimate Pharmacology Study Guide for Nursing Students in 2026 offers deeper insights into the nuances of bedside medication administration.
Monitoring for signs of interaction involves both lab values and clinical symptoms. For anticoagulants, the INR remains the gold standard for tracking Vitamin K interference. For other medications, you must remain vigilant for subtle changes like increased heart rate, new-onset muscle pain, or unexpected GI distress. To refine your clinical judgment and master these scenarios, you can test your knowledge against real-world examples through our Clinical Case Studies.
Mastering Interaction Pharmacology with PharmEDU Resources
Mastering the vast landscape of pharmacology requires more than just reading lists; it demands a structured, visual approach to learning that bridges the gap between theory and practice. While you now understand the mechanisms behind the common drug-food interactions to know, retaining that information for high-stakes exams or clinical rotations is the next challenge. Our High-Yield Video Vignettes help you see the invisible, providing a clear visualization of how furanocoumarins interact with intestinal enzymes or how calcium ions physically trap antibiotic molecules through chelation. These visual aids transform abstract pharmacokinetic concepts into memorable clinical patterns.
To reinforce this knowledge, our Interactive Pharmacology Flashcards allow for rapid-fire drills on the 50 most common drug-food pairs. These tools are designed for micro-learning, enabling you to turn idle minutes between clinical rotations into high-productivity study sessions. When you’re ready to apply your knowledge, our Clinical Case Studies challenge you to act as the primary clinician. You’ll identify subtle dietary triggers in patient histories that could lead to therapeutic failure or toxicity, preparing you for the unpredictable nature of real-world practice.
Exam-Ready Practice Quizzes
Success on standardized exams depends on your ability to decode complex question stems. We provide Pharmacology Practice Quizzes that mirror the complexity of 2026 board standards. Every question includes detailed rationales that explain the PK/PD logic behind the correct answer, ensuring you don’t just memorize the “what” but fully grasp the “why.” If you’re currently in the final stages of your studies, consult The Best NAPLEX Prep Course Guide: How to Pass in 2026 for a comprehensive roadmap to exam success.
Why PharmEDU Beats Traditional Textbooks
Static textbooks often fail to reflect the latest regulatory shifts or the most recent clinical guidelines. PharmEDU provides real-time updates for 2026, ensuring your knowledge remains current with evolving safety standards. Our platform functions as a digital mentor, replacing dry, academic reading with engaging, interactive content that respects your limited time. By focusing on high-yield data and practical application, we remove the administrative burden of tracking your professional development. Excel in your pharmacology coursework with a PharmEDU subscription today!
Elevate Your Clinical Competency in 2026
Mastering the common drug-food interactions to know is a fundamental pillar of safe clinical practice. We’ve examined how understanding pharmacokinetic mechanisms, such as the Cytochrome P450 pathway and chelation, provides a logical framework for predicting adverse events. Moving beyond rote memorization allows you to transition from being a student to a confident practitioner who can provide nuanced patient counseling. These skills are essential for navigating the complex pharmacology sections of your upcoming board exams and for ensuring patient safety in busy outpatient environments.
To support your professional journey, PharmEDU provides a modern suite of learning tools designed by healthcare educators for board exam success. You can access High-Yield Video Vignettes on 100+ topics and utilize our mobile-compliant design for efficient micro-learning between your clinical rotations. This structured approach removes the administrative burden of exam preparation, letting you focus on gaining practical knowledge. Master High-Yield Pharmacology with a PharmEDU Subscription and secure your professional future today. Your commitment to continuous learning is the key to excellence in patient care.
Frequently Asked Questions
How does grapefruit juice interact with so many different medications?
Grapefruit juice contains furanocoumarins that irreversibly inhibit the CYP3A4 enzyme in the small intestine. This mechanism is particularly impactful because CYP3A4 is responsible for metabolizing nearly 50% of all prescription medications. When this enzyme is blocked, the first-pass metabolism of the drug is reduced, which can lead to dangerously high systemic concentrations and increased toxicity.
Can I take my antibiotics with milk or yogurt?
You should avoid taking certain antibiotics, specifically tetracyclines and fluoroquinolones, with dairy products like milk or yogurt. The calcium in these foods binds to the drug molecules in the gastrointestinal tract through a process called chelation. This creates an insoluble complex that prevents the medication from being absorbed into the bloodstream, which may result in the failure of the antibiotic treatment.
Why is it dangerous to eat spinach while taking Warfarin?
Eating large amounts of spinach is dangerous for patients on Warfarin because the high Vitamin K content directly antagonizes the drug’s anticoagulant effect. Warfarin works by inhibiting the synthesis of Vitamin K-dependent clotting factors. While you don’t need to eliminate spinach entirely, you must maintain a consistent daily intake to prevent your INR from fluctuating and increasing the risk of blood clots.
What is a Disulfiram-like reaction and which drugs cause it?
A Disulfiram-like reaction occurs when medications like Metronidazole or Tinidazole inhibit the enzyme acetaldehyde dehydrogenase, leading to a toxic buildup of acetaldehyde. If a patient consumes alcohol while taking these drugs, they will experience distressing symptoms such as severe flushing, nausea, vomiting, and a rapid heartbeat. This reaction can occur even with small amounts of alcohol found in some mouthwashes or cough syrups.
How long should I wait between eating and taking a medication that requires an empty stomach?
You should wait at least one hour before eating or two hours after a meal to ensure a medication is taken on an empty stomach. This timing is one of the most common drug-food interactions to know because it ensures that food does not interfere with the drug’s solubility or absorption rate. Following this rule helps maintain the expected therapeutic levels of the medication in your system.
Are there any common foods that interact with ACE inhibitors?
ACE inhibitors can interact with potassium-rich foods such as bananas, oranges, and potassium-based salt substitutes. These medications naturally cause the body to retain potassium by inhibiting aldosterone. If you consume excessive amounts of high-potassium foods while on an ACE inhibitor, you risk developing hyperkalemia, which can lead to serious cardiac arrhythmias or muscle weakness.
What are the symptoms of a hypertensive crisis caused by tyramine?
The symptoms of a tyramine-induced hypertensive crisis typically include a sudden, severe occipital headache and palpitations. You might also experience neck stiffness, nausea, vomiting, and a dangerously elevated blood pressure. Recognizing these signs is essential for those studying the common drug-food interactions to know, as this crisis requires immediate medical intervention to prevent cardiovascular or neurological damage.
Is it safe to take multivitamins with my prescription drugs?
Taking multivitamins with prescription drugs is not always safe because minerals like iron, magnesium, and calcium can interfere with drug absorption. These components often cause chelation or alter the gastric pH, which changes how the body processes your primary medication. It’s best to consult with a healthcare professional to see if you need to stagger your multivitamin dose several hours away from your prescriptions.