Autonomic Nervous System Pharmacology Review: High-Yield Guide for 2026
With nearly 50% of hypertension patients in the United States failing to reach their blood pressure goals despite multiple treatments, the traditional approach to autonomic pharmacology is clearly hitting a ceiling. You likely feel this complexity every time you sit down to study. It’s easy to feel overwhelmed by the sheer volume of drug classes or find yourself mixing up sympathetic and parasympathetic effects during a high-stakes exam. This autonomic nervous system pharmacology review shifts your focus from rote memorization to mastering receptor geography, ensuring you can navigate these challenges with precision.
We’ll provide you with a structured framework to predict clinical outcomes based on core physiological principles rather than static lists. You’ll gain a clear understanding of receptor locations and the clinical confidence required to pass your pharmacology board exams. We’ll also examine critical 2026 developments, such as the anticipated Q2 approval of the first-in-class aldosterone synthase inhibitor, baxdrostat, and the resubmission status of sublingual epinephrine films. To reinforce these concepts, you can utilize our Interactive Pharmacology Flashcards and High-Yield Video Vignettes to bridge the gap between theory and professional practice.
Key Takeaways
- Identify the core mechanisms of dual innervation to understand how the sympathetic and parasympathetic systems regulate involuntary functions.
- Navigate this autonomic nervous system pharmacology review to master receptor selectivity and classify direct or indirect-acting cholinergic and adrenergic agents.
- Develop the ability to predict clinical outcomes and side effects by mapping specific receptor actions to the heart, lungs, and gastrointestinal tract.
- Analyze complex hemodynamic responses, including reflex tachycardia and bradycardia, to solve high-yield clinical case scenarios efficiently.
- Enhance your exam readiness by leveraging high-yield video vignettes and interactive flashcards designed for professional-grade retention and board success.
Foundations of Autonomic Nervous System Pharmacology
The autonomic nervous system serves as the master regulator for involuntary physiological processes, maintaining homeostasis by controlling cardiac output, vascular tone, and digestive motility. Mastering this system is more than an academic exercise; it’s the essential gateway to understanding cardiovascular and respiratory pharmacology. Without a firm grasp of how these pathways interact, predicting how a patient will respond to a beta-blocker or a bronchodilator becomes nearly impossible. This autonomic nervous system pharmacology review focuses on the structural logic that governs these responses to help you move beyond rote memorization.
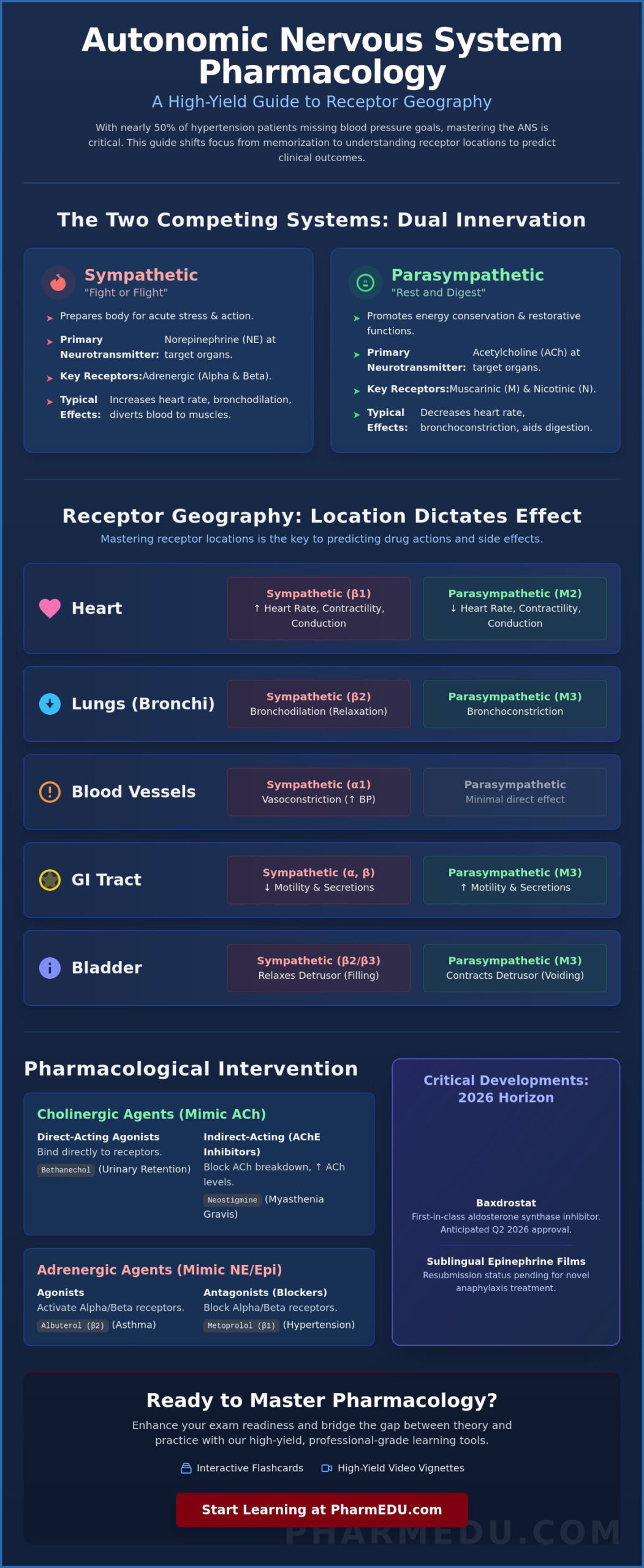
Most organs receive dual innervation, meaning they’re influenced by both the sympathetic (fight or flight) and parasympathetic (rest and digest) divisions. These systems typically act in opposition. While the sympathetic system prepares the body for acute stress by increasing heart rate and diverting blood to skeletal muscles, the parasympathetic system promotes energy conservation and restorative functions. Understanding this balance allows you to predict side effects; a drug that blocks one system often allows the effects of the other to dominate. The architecture of the ANS relies on a two-neuron chain. Preganglionic fibers originate in the central nervous system and synapse at a ganglion, where they release acetylcholine (ACh) to activate postganglionic fibers. These postganglionic neurons then travel to the target organ to release the final neurotransmitter. This structural consistency is why certain drugs have widespread, systemic effects while others remain localized.
Neurotransmitters: Acetylcholine and Norepinephrine
The distinction between cholinergic and adrenergic transmission defines the two primary branches of ANS pharmacology. Acetylcholine mediates cholinergic transmission across all preganglionic synapses and parasympathetic postganglionic synapses. In contrast, norepinephrine and epinephrine drive adrenergic transmission at most sympathetic postganglionic junctions. To maintain precise control, the body uses specific enzymes like acetylcholinesterase (AChE) to degrade ACh, while monoamine oxidase (MAO) and catechol-O-methyltransferase (COMT) handle the breakdown of catecholamines. The synaptic cleft is the primary site of pharmacological intervention where drugs either mimic, block, or prolong the life of these neurotransmitters.
Receptor Geography: Where Drugs Actually Act
Receptor location is the most high-yield concept for any clinician. Muscarinic receptors (M1-M3) primarily handle parasympathetic effects, with M2 located in the heart and M3 found in smooth muscle and glands. Nicotinic receptors (Nn, Nm) are found at autonomic ganglia and the neuromuscular junction. Adrenergic receptors are equally specific: Alpha-1 receptors reside in vascular smooth muscle, Alpha-2 receptors often act as presynaptic brakes, Beta-1 receptors dominate the heart, and Beta-2 receptors facilitate bronchodilation in the lungs. The high-yield rule is simple: receptor location dictates the drug’s clinical effect. If you know where the receptor lives, you don’t have to memorize a list of actions; you can derive them through physiology. Our Interactive Pharmacology Flashcards are specifically designed to help you internalize these locations through active recall and repetition.
Cholinergic Pharmacology: Parasympathetic Modulation
Cholinergic pharmacology focuses on drugs that mimic or inhibit the actions of acetylcholine, the primary neurotransmitter of the parasympathetic nervous system. This is a cornerstone of any autonomic nervous system pharmacology review. We classify these agents into two main groups. Direct-acting agonists bind directly to muscarinic or nicotinic receptors to elicit a response. For example, Bethanechol is a muscarinic agonist frequently used for non-obstructive urinary retention, while Pilocarpine remains a staple for treating glaucoma by facilitating aqueous humor drainage. These drugs provide targeted therapy by acting where the receptors are most concentrated.
Indirect-acting drugs, known as acetylcholinesterase (AChE) inhibitors, work by preventing the breakdown of endogenous acetylcholine in the synaptic cleft. Students often struggle with why these “indirect” drugs cause such widespread systemic effects. The reason is simple; AChE is present at every cholinergic synapse, including autonomic ganglia, the neuromuscular junction, and all parasympathetic postganglionic junctions. By inhibiting this enzyme, you increase ACh levels globally. This mechanism is vital for managing Myasthenia Gravis with agents like Neostigmine, which improves muscle strength, or slowing the progression of Alzheimer’s disease with Donepezil by enhancing central cholinergic tone.
Muscarinic Antagonists (Anticholinergics)
Anticholinergics like Atropine, Ipratropium, and Oxybutynin work by competitively blocking muscarinic receptors, effectively turning off the “rest and digest” signal. Atropine is the primary choice for symptomatic bradycardia, as it blocks the M2 receptors in the heart to increase rate. Ipratropium provides targeted bronchodilation for COPD patients, while Oxybutynin reduces bladder spasms in patients with overactive bladder. When using these, it’s helpful to compare their side-effect profiles with other common cardiac medications, as seen in our ACE Inhibitors Pharmacology Guide. Overdose leads to the classic anticholinergic syndrome, often remembered by the mnemonic “Dry as a bone, Red as a beet” to describe the lack of secretions and cutaneous vasodilation.
Cholinergic Crisis vs. Myasthenic Crisis
Distinguishing between these two conditions is a favorite board exam topic because the clinical presentations can overlap. A cholinergic crisis results from excessive ACh, often due to organophosphate poisoning. It’s characterized by the SLUDGE (Salivation, Lacrimation, Urination, Defecation, GI distress, Emesis) or DUMBBELS (Diarrhea, Urination, Miosis, Bradycardia, Bronchospasm, Emesis, Lacrimation, Salivation) mnemonics. The Tensilon test uses Edrophonium, a very short-acting AChE inhibitor, to differentiate them. If the patient’s muscle weakness improves, it’s a myasthenic crisis; if it worsens, it’s a cholinergic crisis. According to recent updates in Autonomic Pharmacology, managing these emergencies in 2026 still relies on Atropine for symptom control and Pralidoxime as the specific regenerator for the enzyme. To master these high-stakes scenarios, you can test your knowledge with our Interactive Pharmacology Flashcards.
Adrenergic Pharmacology: Sympathetic System Mastery
Adrenergic pharmacology centers on the sympathetic nervous system’s response to stress and environmental demands. While cholinergic drugs often target localized organ functions, adrenergic agents trigger widespread physiological shifts. Mastering this branch requires a precise understanding of receptor selectivity. This Autonomic Nervous System Pharmacology Review highlights how drugs are categorized by their affinity for Alpha and Beta receptors, which dictates their therapeutic use and potential side-effect profiles.
Epinephrine remains the non-selective gold standard for treating anaphylaxis. It stimulates Alpha-1, Beta-1, and Beta-2 receptors simultaneously, addressing hypotension, myocardial depression, and bronchoconstriction in a single intervention. As of 2026, the landscape for administration is evolving toward more patient-friendly options. Although the FDA issued a Complete Response Letter for the sublingual epinephrine film Anaphylm in early 2026 due to packaging concerns, a resubmission is planned for the third quarter of 2026. This reflects a broader industry trend toward non-invasive delivery methods for autonomic emergencies.
Selective Alpha-agonists serve distinct clinical roles. Phenylephrine acts primarily on Alpha-1 receptors to cause vasoconstriction, making it effective for nasal congestion or maintaining blood pressure during anesthesia. In contrast, Clonidine is an Alpha-2 agonist that acts centrally to reduce sympathetic outflow, lowering blood pressure in hypertensive patients. Beta-2 agonists like Albuterol focus on the respiratory system. They trigger bronchodilation by relaxing airway smooth muscle. High doses can cause metabolic side effects like hypokalemia or tremors due to skeletal muscle stimulation. You can refine your ability to predict these outcomes with our Pharmacology Practice Quizzes.
Beta-Adrenergic Antagonists (Beta-Blockers)
Clinicians must differentiate between cardioselective and non-selective beta-blockers to ensure patient safety. Cardioselective agents like Metoprolol and Atenolol primarily target Beta-1 receptors in the heart. This makes them safer for patients with hypertension who also have underlying respiratory issues. Non-selective blockers like Propranolol affect both Beta-1 and Beta-2 receptors. Because Beta-2 blockade causes bronchoconstriction, these drugs are strictly contraindicated in patients with asthma or COPD. These medications are high-yield staples for board exams because they require a deep understanding of receptor geography.
Alpha-Blockers and Mixed Antagonists
Alpha-blockers like Prazosin and Tamsulosin are essential for managing hypertension and Benign Prostatic Hyperplasia (BPH). By blocking Alpha-1 receptors, they relax vascular and prostatic smooth muscle to improve flow. Labetalol and Carvedilol offer a unique mixed action by blocking both Alpha and Beta receptors; this is particularly useful in hypertensive emergencies where rapid, balanced pressure reduction is required. Patients starting alpha-blockers must be warned about the first-dose phenomenon, which is a sudden, severe drop in blood pressure that can lead to syncope shortly after the initial dose.
High-Yield ANS Comparison and Clinical Scenarios
Mastering autonomic pharmacology isn’t about memorizing isolated drug names; it’s about understanding the physiological tug-of-war between two opposing systems. Most board exams, including the NAPLEX and USMLE, move beyond simple definitions to test your ability to predict how the body compensates for pharmacological interventions. The baroreceptor reflex is a frequent trap for students. If a drug causes systemic vasoconstriction through Alpha-1 stimulation, the body responds with reflex bradycardia to maintain homeostasis. Conversely, a vasodilator drops peripheral resistance and triggers reflex tachycardia. Recognizing these patterns is essential for any autonomic nervous system pharmacology review, as it allows you to predict physiological compensations that aren’t listed on a standard drug label.
The “Fight or Flight” vs. “Rest and Digest” Cheat Sheet
Contrast is the most effective tool for long-term retention. When evaluating drug effects on major organ systems, use these direct comparisons to guide your clinical reasoning:
- The Eye: Sympathetic activation causes mydriasis (pupillary dilation) via Alpha-1 receptors; parasympathetic activation leads to miosis (pupillary constriction) via M3 receptors.
- The Lungs: Sympathetic stimulation triggers bronchodilation through Beta-2 receptors. The parasympathetic system causes bronchoconstriction and increased secretions through M3 receptors.
- The Heart: Sympathetic signals increase heart rate and contractility through Beta-1 receptors. Parasympathetic signals decrease heart rate via M2 receptors.
- The GI Tract: The sympathetic system slows motility and constricts sphincters, while the parasympathetic system increases motility and relaxes sphincters to promote digestion.
Common ANS Drug-Drug Interactions
Clinical safety requires a deep understanding of how different autonomic agents interact. Combining a Beta-blocker with a Beta-agonist is often clinically counterproductive, as the antagonist directly prevents the agonist from reaching its target receptor. You must also be vigilant about the “anticholinergic burden”. This occurs when a patient takes multiple medications with secondary anticholinergic effects, such as a TCA for depression and an antihistamine for allergies. In the elderly, this cumulative effect significantly increases the risk of cognitive impairment, falls, and urinary retention. Applying these high-yield concepts to real-world scenarios with our Clinical Case Studies will help you bridge the gap between theory and professional practice.
For those looking to expand their knowledge beyond the ANS, our Comprehensive Pharmacology Guide provides a wider view of drug-receptor interactions. This broader context ensures that your autonomic nervous system pharmacology review remains integrated with other critical drug classes, such as those affecting the renal and central nervous systems.
Optimizing Your ANS Review with PharmEDU’s High-Yield Resources
Static textbooks often struggle to convey the dynamic nature of receptor-ligand interactions. This autonomic nervous system pharmacology review has mapped the structural geography of the ANS, but long-term retention requires a shift from passive reading to active engagement. PharmEDU’s micro-learning approach addresses this by breaking down complex adrenergic and cholinergic pathways into concise, high-impact modules. By focusing on specific receptor subtypes in isolation before integrating them into systemic circuits, you can build a comprehensive mental map without the cognitive overload typically associated with this subject.
Visualizing how a non-selective drug like Epinephrine interacts with multiple receptors is simplified through our High-Yield Video Vignettes. These vignettes provide a clear, visual narrative of physiological changes, making it easier to predict clinical outcomes during an exam or in a clinical setting. To reinforce this knowledge, our Interactive Pharmacology Flashcards utilize active recall to help you internalize drug names and receptor affinities. In 2026, flexibility is essential; our platform is fully mobile-compliant, allowing you to conduct a high-yield study session during a clinical rotation or a morning commute.
Beyond the Textbook: Interactive ANS Learning
The transition from theory to clinical practice is often the steepest part of the learning curve. Our Pharmacology Practice Quizzes are designed to mimic the rigor and format of the NAPLEX Prep Course, ensuring you’re prepared for the specific phrasing and complexity of board-level questions. Beyond standardized testing, our Clinical Case Studies challenge you to apply your autonomic nervous system pharmacology review to real-world patient care scenarios. You’ll analyze hemodynamic shifts and drug-drug interactions in a risk-free digital environment. Join the thousands of healthcare students who have moved past rote memorization to achieve true clinical confidence with PharmEDU.
Start Your Professional Pharmacology Journey
Success in pharmacology isn’t an accident; it’s the result of a structured, methodical study plan. Whether you’re preparing for medical boards or seeking specialized knowledge through our Pharmacology Study Guide for Nursing Students, having the right tools makes a measurable difference in your performance. We offer flexible options to fit your career stage, including a PharmEDU Monthly Subscription for short-term intensive review or a PharmEDU Annual Subscription for year-round support. For educational organizations, our Institutional Platform License provides a comprehensive solution for entire cohorts. Invest in your professional development today and secure the scores you need to advance your career.
Elevating Your Clinical Expertise for 2026
Mastering the autonomic nervous system is the cornerstone of safe and effective prescribing. By focusing on receptor geography rather than rote lists, you’ve gained the ability to predict clinical outcomes and manage complex drug interactions with precision. This autonomic nervous system pharmacology review has bridged the gap between physiological theory and the emerging clinical realities of 2026. Whether you’re navigating the nuances of cholinergic crises or preparing for the next wave of drug approvals, your commitment to structured learning is the key to professional excellence.
PharmEDU supports your journey with a mobile-compliant micro-learning platform designed for busy professionals. Our resources cover over 100 high-yield topics and are trusted by top-tier pharmacy and nursing programs globally. You don’t have to face these academic challenges alone. Take the next step in your professional development by accessing the tools used by the industry’s best.
Master ANS Pharmacology Today with PharmEDU Subscriptions
Your path to board exam success and clinical mastery is well within reach. Stay focused, stay curious, and continue to build the expertise your patients deserve.
Frequently Asked Questions
What is the easiest way to remember the Autonomic Nervous System receptors?
The most effective method is to link the receptor number to the organ’s anatomy. You’ve only got one heart (Beta-1) and two lungs (Beta-2). This autonomic nervous system pharmacology review suggests using the “QISS” and “QIQ” mnemonics to master G-protein linkages. Once you know the receptor’s location and its signaling pathway, you can logically derive the drug’s effect without relying on rote memorization of long lists.
How do cholinergic drugs differ from adrenergic drugs in their mechanism of action?
Cholinergic drugs work by mimicking or increasing the levels of acetylcholine at muscarinic and nicotinic receptors to promote “rest and digest” activities. Adrenergic drugs target the sympathetic system by activating Alpha or Beta receptors, usually through norepinephrine or epinephrine pathways. While cholinergic agents focus on increasing secretions and GI motility, adrenergic agents are designed to increase cardiac output and facilitate bronchodilation during stress responses.
What are the most common side effects of anticholinergic medications?
Anticholinergic side effects result from the systemic blockade of muscarinic receptors, leading to decreased parasympathetic tone. You’ll commonly see patients reporting dry mouth, blurred vision, constipation, and urinary retention. In clinical practice, it’s vital to monitor for more severe central effects like confusion or hallucinations, especially in elderly patients. These individuals are more sensitive to the cumulative “anticholinergic burden” from multiple medications like antihistamines or tricyclic antidepressants.
Why are Beta-2 agonists used for asthma treatment instead of Beta-1 agonists?
Beta-2 agonists are the standard for asthma because they selectively target receptors in the bronchial smooth muscle to cause bronchodilation. Beta-1 receptors are almost exclusively found in the heart. If you used a Beta-1 agonist for a respiratory issue, it’d cause dangerous tachycardia and increased myocardial oxygen demand without opening the airways. Selective Beta-2 drugs allow for effective respiratory relief while minimizing these unwanted cardiovascular side effects.
What is the difference between a cholinergic crisis and a myasthenic crisis?
A cholinergic crisis involves an overstimulation of the neuromuscular junction due to excess acetylcholine, whereas a myasthenic crisis is caused by a severe lack of acetylcholine. Clinicians use the Tensilon test to tell them apart. If a patient’s muscle strength improves after receiving edrophonium, it’s a myasthenic crisis. If the weakness worsens, it’s a cholinergic crisis, which requires the immediate cessation of anticholinesterase drugs and the administration of atropine.
Which ANS drugs are most likely to appear on the NAPLEX or NCLEX exams in 2026?
Expect a heavy focus on first-in-class therapies like baxdrostat, which is anticipated for FDA approval in the second quarter of 2026. This autonomic nervous system pharmacology review also identifies sublingual epinephrine films as a high-yield topic following their planned resubmission in late 2026. Traditional staples like metoprolol, albuterol, and organophosphate reversal agents remain essential. Board exams frequently test these drugs through complex clinical vignettes rather than simple identification.
Can I use PharmEDU to study for pharmacology institutional exams?
Yes, PharmEDU is specifically designed to support students through both national boards and localized institutional exams. Our Institutional Platform License provides universities with a structured way to track student progress across high-yield topics. You can use our Interactive Pharmacology Flashcards and Practice Quizzes to simulate the specific rigor of your department’s assessments. It’s a reliable way to ensure you’re fully prepared for the administrative and scientific requirements of your professional program.