Anxiolytics and Hypnotics Review: High-Yield Pharmacology for Healthcare Students (2026)
What if your ability to distinguish between a therapeutic sedative and a fatal overdose depended entirely on understanding the millisecond-level kinetics of a single chloride channel? For many healthcare students, the pharmacological landscape of GABA-A modulators feels like an endless list of “pam” and “lam” suffixes that blur together during high-stakes board exams. It’s exhausting to struggle with overlapping side effect profiles when you’re trying to master this anxiolytics and hypnotics review for clinical practice.
We understand that rote memorization isn’t enough to navigate modern medicine, especially with the 2026 regulatory landscape shifting rapidly. This guide promises to transform your understanding of sedative-hypnotic mechanisms, giving you the confidence to tackle complex clinical cases and board questions. We’ll preview the essential distinctions between drug classes, including the recent permanent Schedule I classification of five synthetic benzodiazepines and the rise of non-GABAergic treatments like orexin antagonists. By focusing on chloride channel frequency versus duration, you’ll gain a logical framework that replaces memorization with professional expertise.
Key Takeaways
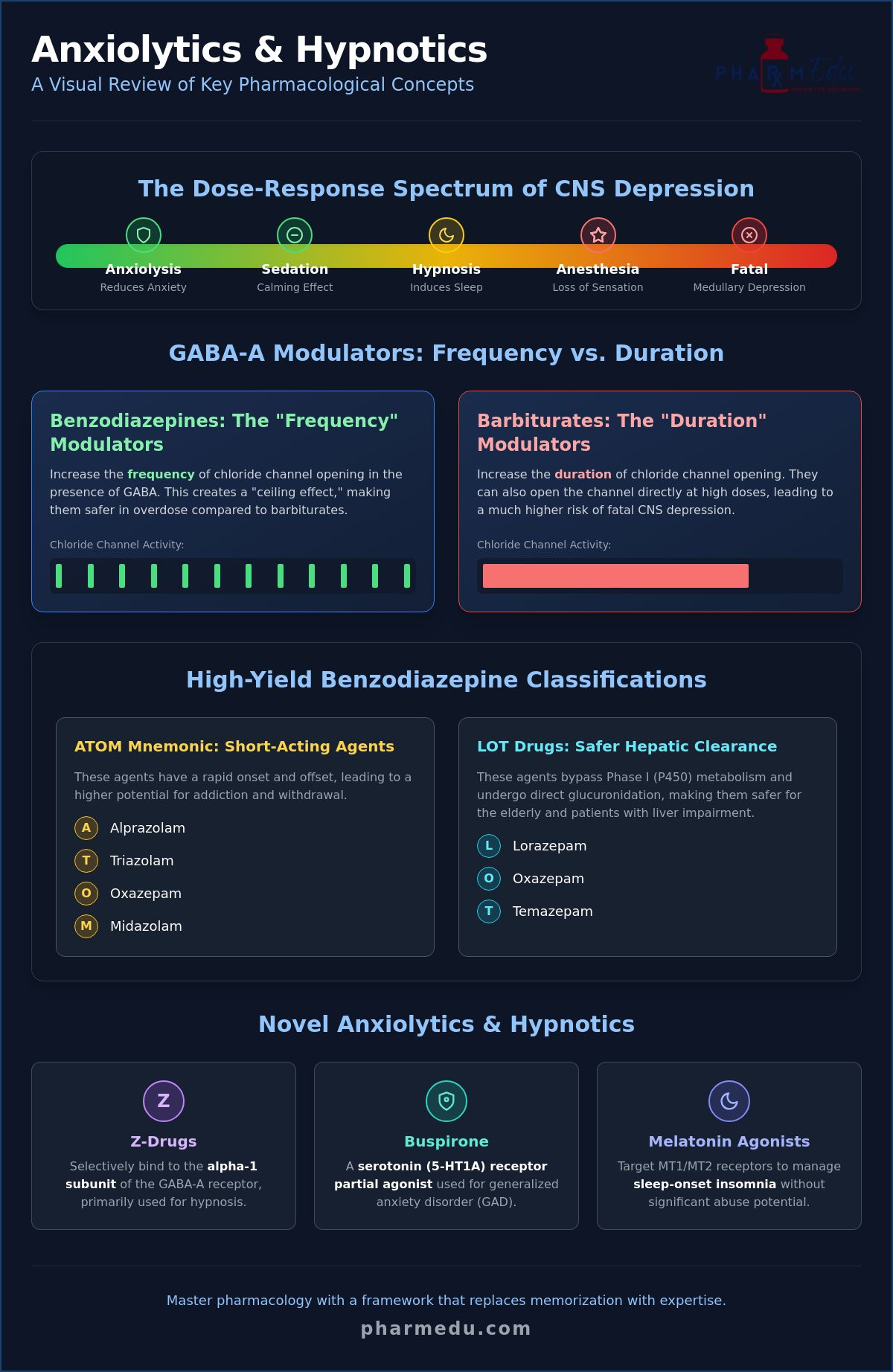
- Define the dose-response curve to understand the progression from simple anxiolysis to hypnosis and surgical anesthesia across different drug classes.
- Master the ATOM mnemonic to categorize benzodiazepines by their half-life, ensuring precise selection for short, intermediate, or long-acting clinical needs.
- Differentiate between GABA-A modulators by contrasting the “frequency” rule of benzodiazepines with the “duration” rule of barbiturates and the alpha-1 selectivity of Z-drugs.
- Identify the clinical roles of non-GABAergic agents, including Buspirone for generalized anxiety and melatonin receptor agonists for sleep-onset insomnia.
- Utilize this anxiolytics and hypnotics review to navigate high-yield board exam distractors and clinical vignettes with professional confidence.
Understanding the Sedative-Hypnotic Spectrum and Drug Classification
The pharmacological management of the central nervous system (CNS) requires a precise understanding of the dose-response relationship. This anxiolytics and hypnotics review begins with the fundamental concept that CNS depression occurs on a continuum. At lower doses, these agents reduce pathological anxiety, a state known as anxiolysis, without significantly impairing motor or mental functions. As the dose increases, the effect progresses through sedation, hypnosis, and eventually surgical anesthesia. If the dose reaches toxic levels, medullary depression can lead to respiratory failure and death. This predictable progression is why clinicians must respect the potency and pharmacokinetics of each individual agent.
Sedative-hypnotics are primarily classified by their chemical structure and receptor interaction. The three main pillars of this class include benzodiazepines, barbiturates, and non-benzodiazepine hypnotics. Beyond these, modern medicine utilizes melatonin receptor agonists and serotonin receptor partial agonists to achieve specific clinical outcomes. These medications are indispensable for managing acute anxiety disorders, chronic insomnia, and certain types of seizure activity. However, the risk of global CNS depression remains a critical consideration, especially when multiple agents are combined or when using older drug classes with narrower therapeutic windows.
The GABA-A Receptor: The Primary Target
The GABA-A receptor is a pentameric ligand-gated chloride channel, typically composed of two alpha, two beta, and one gamma subunit. When the inhibitory neurotransmitter GABA binds to the receptor, it triggers a chloride influx that leads to neuronal hyperpolarization. This shift in electrical potential makes the neuron less likely to fire an action potential, effectively “quieting” the nervous system. While benzodiazepines and barbiturates both enhance this inhibitory effect, they bind to distinct allosteric sites on the receptor complex. These structural nuances explain why their clinical profiles and safety margins differ so drastically in a hospital setting.
Anxiolytics vs. Hypnotics: Clinical Distinctions
The distinction between an anxiolytic and a hypnotic often depends more on the dose and pharmacokinetics than the drug class itself. Anxiolytics aim to reduce symptoms of tension with minimal sedation, allowing for normal daytime activity. In contrast, this Hypnotic drugs overview highlights their primary role in sleep induction and maintenance. For instance, a low dose of a benzodiazepine might treat a panic attack, while a higher dose of the same agent serves as a pre-surgical sedative. The sedative-hypnotic continuum represents a progressive depth of CNS depression where the clinical outcome is determined by the specific drug’s efficacy and the administered dose.
Benzodiazepines: Mechanism of Action, Pharmacokinetics, and Clinical Pearls
Benzodiazepines (BZDs) remain the most frequently prescribed class in any anxiolytics and hypnotics review, primarily due to their favorable safety profile compared to older agents. Their mechanism relies on positive allosteric modulation of the GABA-A receptor. Unlike barbiturates, BZDs don’t open the chloride channel directly. Instead, they increase the frequency of channel opening in the presence of GABA. This subtle distinction provides a “ceiling effect” that makes isolated BZD overdoses less likely to cause fatal respiratory depression than barbiturates. It’s a fundamental concept that defines their clinical utility across various medical specialties.
Pharmacokinetic classification is vital for board exams and safe prescribing. Students often use the ATOM mnemonic (Alprazolam, Triazolam, Oxazepam, Midazolam) to remember short-acting agents, which have a higher addiction potential due to rapid onset and offset. For patients with hepatic impairment or the elderly, clinicians prioritize the “LOT” drugs: Lorazepam, Oxazepam, and Temazepam. These agents undergo direct glucuronidation, bypassing Phase I cytochrome P450 metabolism, which ensures safer clearance when liver function is compromised. If you’re struggling to keep these metabolic pathways straight, our Interactive Pharmacology Flashcards provide a structured way to drill these high-yield facts.
Common adverse effects include daytime sedation and anterograde amnesia, which can be particularly problematic in geriatric populations. While BZDs are generally safer than alternatives, they can cause significant respiratory depression when combined with other CNS depressants like alcohol or opioids. This Anxiolytics and Sedative-Hypnotics Review details how these risks scale with dosage and patient age, providing a deeper look at the toxicology involved.
High-Yield Benzodiazepine Indications
BZDs are first-line for acute management of panic attacks and severe anxiety, though long-term use is discouraged due to the risk of tolerance and dependence. In emergency medicine, intravenous Lorazepam or Diazepam is the gold standard for breaking status epilepticus. For alcohol withdrawal syndrome, long-acting agents like Chlordiazepoxide and Diazepam are preferred because their long half-lives provide a self-tapering effect that helps prevent seizures and delirium tremens during the detoxification process.
Antidote and Overdose Management
Flumazenil acts as a competitive antagonist at the BZD binding site, making it the specific antidote for BZD-induced sedation. However, clinicians must use it with extreme caution. It’s often contraindicated in chronic BZD users or patients with unknown ingestions because rapidly reversing BZD effects can precipitate life-threatening withdrawal seizures. When managing a suspected overdose, it’s essential to distinguish BZD toxicity from opioid overdose; look for the absence of miosis (pinpoint pupils) and the lack of response to Naloxone to confirm your clinical suspicion.
Comparing Barbiturates and Non-Benzodiazepine “Z-Drugs”
A comprehensive anxiolytics and hypnotics review must address the stark contrast between the older barbiturate class and the modern non-benzodiazepine “Z-drugs.” While benzodiazepines act by increasing the frequency of chloride channel opening, barbiturates function by increasing the duration of these openings. This physiological nuance has profound clinical consequences. Unlike benzodiazepines, barbiturates can activate the GABA-A receptor even in the absence of GABA at high concentrations. This lack of a “ceiling effect” explains their extremely low therapeutic index and why they’ve been largely replaced in routine practice by safer alternatives.
The development of Z-drugs, including Zolpidem, Zaleplon, and Eszopiclone, represents a significant leap in sleep medicine. These agents are technically non-benzodiazepines but bind to the same BZD site on the GABA-A receptor. Their advantage lies in their selectivity for the alpha-1 subunit, which is primarily responsible for sedation. This specificity allows them to induce sleep with minimal disruption to the patient’s sleep architecture, preserving REM and deep sleep stages more effectively than traditional benzodiazepines. Understanding the pharmacology of anxiolytics and hypnotics is essential for recognizing why Z-drugs are now the preferred first-line pharmacological intervention for short-term insomnia.
Barbiturates: High-Yield Risks and Inductions
Barbiturates like Phenobarbital are still utilized for specific seizure disorders, but their side effect profile is a minefield for clinicians. They’re potent inducers of the Cytochrome P450 enzyme system. This means they significantly accelerate the metabolism of other drugs, such as Warfarin or oral contraceptives, often leading to therapeutic failure of the co-administered medication. A classic board exam “trap” involves Acute Intermittent Porphyria; barbiturates induce delta-aminolevulinate (ALA) synthase, which can precipitate a life-threatening porphyria crisis. Their ability to cause profound respiratory and cardiovascular depression makes them far more dangerous in overdose scenarios than Z-drugs or benzodiazepines.
Z-Drugs: Modern Management of Insomnia
When selecting a Z-drug, the patient’s specific sleep complaint dictates the choice. Zolpidem has a moderate half-life, making it suitable for sleep maintenance, whereas Zaleplon has an ultra-short half-life, ideal for patients who only struggle with sleep onset or wake up in the middle of the night. Despite their improved safety, these drugs aren’t without risks. They’re notorious for causing “complex sleep behaviors,” such as sleep-walking or even sleep-driving, which can occur even after a single dose. A helpful pharmacology study tip for your next exam: remember “Z-drugs for Zzz” to recall their alpha-1 selectivity and primary role as hypnotics rather than anxiolytics.
Novel Anxiolytics and Hypnotics: Beyond the GABA Receptor
As we look toward 2026, the pharmacological landscape is expanding well beyond the traditional GABA receptor. This anxiolytics and hypnotics review highlights a significant shift toward targeted neurotransmitter systems that minimize the global CNS depression seen with older agents. With the anticipated FDA consideration of novel treatments like MM120 for Generalized Anxiety Disorder and Fasedienol nasal spray for social anxiety, the options for non-sedating therapy are growing. These advancements allow clinicians to treat symptoms while preserving the patient’s cognitive clarity and reducing the risk of dependency.
Buspirone: The Non-Sedating Alternative
Buspirone remains the classic example of a non-sedating anxiolytic. It functions as a 5-HT1A partial agonist, meaning it doesn’t interact with the GABA-A receptor complex at all. This lack of GABAergic activity is precisely why it doesn’t cause the “buzz” or cognitive impairment associated with benzodiazepines. A critical clinical pearl for board exams is the 1-2 week lag time required for its therapeutic effects to manifest. It’s not suitable for acute panic attacks, but it’s an excellent choice for long-term GAD management in patients with a history of substance use disorders, as it lacks abuse potential and withdrawal symptoms.
Ramelteon and Suvorexant: Targeting Circadian Rhythms
Sleep medicine has also evolved with agents like Ramelteon and Suvorexant. Ramelteon is a melatonin receptor agonist that mimics the body’s natural “darkness signal” by targeting MT1 and MT2 receptors in the suprachiasmatic nucleus. It’s specifically indicated for sleep-onset insomnia and doesn’t carry a risk of rebound insomnia. On the other hand, Suvorexant targets the arousal system directly. Orexin receptor antagonists promote sleep by blocking the binding of wake-promoting neuropeptides to their receptors in the lateral hypothalamus, effectively turning off the body’s primary arousal signal.
While newer agents are gaining ground, older drugs like Trazodone and Hydroxyzine are frequently used off-label for their sedative properties. Trazodone, an antidepressant with 5-HT2 and H1 blocking properties, has actually become the most commonly prescribed hypnotic medication due to its lack of addiction potential. Similarly, Hydroxyzine, a first-generation antihistamine, is often used for short-term anxiety relief when benzodiazepines are contraindicated. Understanding these diverse pathways is essential for modern clinical practice. To see these mechanisms in action through clinical scenarios, explore our Clinical Case Studies.
Mastering Sedative-Hypnotic Pharmacology for Board Certification
Success on professional licensing exams requires more than just knowing drug names. It demands an ability to synthesize mechanisms and clinical presentations under pressure. This anxiolytics and hypnotics review concludes by focusing on the application of these concepts in clinical vignettes. Examiners often test your ability to select the safest agent for specific populations. For instance, if a vignette describes an elderly patient with liver cirrhosis and insomnia, the correct answer isn’t just any sedative; it’s a “LOT” drug like Oxazepam that avoids Phase I metabolism. Recognizing these patterns is the difference between a passing score and professional mastery.
Board questions frequently use distractors to test your understanding of contraindications. A common board “trap” involves a patient with a history of chronic benzodiazepine use presenting with an overdose. While Flumazenil is the specific antidote, choosing it in this context is often incorrect because it can precipitate life-threatening seizures. Similarly, you must stay updated on regulatory shifts. As of April 1, 2026, five synthetic benzodiazepines, including Clonazolam and Etizolam, are permanently placed in Schedule I. This regulatory fact may appear in questions regarding high-potency toxicities or the strictest levels of legal control.
High-Yield Board Mnemonics and Comparisons
Mnemonics remain an essential tool for active recall during the USMLE or NAPLEX. To remember receptor binding, use “B-D-Z”: Benzodiazepines bind to a Different site than GABA, and Zolpidem is similar in its binding location. The most critical distinction for chloride channel kinetics is the “Duration vs. Frequency” rule. Remember “Barbi-dur-ate” for increased duration of channel opening and “Ben-fre-diazepine” for increased frequency. These distinctions are high-yield because they explain why barbiturates lack the safety ceiling seen with benzodiazepines, making them far more dangerous in a clinical overdose scenario.
Beyond the Textbook: Interactive Learning
Static reading often fails to build the clinical intuition needed for modern exams. PharmEDU bridges this gap by utilizing high-yield video vignettes that visually demonstrate molecular mechanisms. Instead of just reading about 5-HT1A partial agonism, you can see how Buspirone interacts with the synapse in real-time, which solidifies your understanding of why it lacks immediate effect.
Consistent practice with pharmacology practice quizzes ensures that these distinctions move from short-term memory to long-term retention. For those approaching their final certification, our NAPLEX prep course guide provides an integrated study plan that balances sedative-hypnotic review with other high-stakes topics. This structured approach helps you navigate the evolving regulatory environment and scientific results of 2026 with professional confidence and precision.
Elevate Your Clinical Mastery in 2026
Mastering the intricacies of the GABA-A receptor and the evolving regulatory landscape of sedative-hypnotics is a cornerstone of professional excellence. This anxiolytics and hypnotics review has provided you with the foundational tools to distinguish between chloride channel kinetics and the selective binding of modern Z-drugs. By moving beyond rote memorization and focusing on these high-yield distinctions, you’re not just preparing for an exam; you’re developing the precision required for safe patient care in an increasingly complex pharmacological environment.
To further solidify your knowledge, start your high-yield pharmacology review with PharmEDU today. Our platform features over 100 high-yield topics delivered through mobile-compliant micro-learning segments, all designed by healthcare educators for board exam success. Whether you’re drilling mechanisms with interactive flashcards or testing your logic with clinical case studies, we’re here to ensure you approach your boards with absolute confidence. Your journey toward clinical expertise is a marathon, and we’re proud to be your partner in every mile.
Frequently Asked Questions
What is the primary difference between benzodiazepines and barbiturates?
The primary difference lies in their effect on the GABA-A chloride channel. Benzodiazepines increase the frequency of channel opening, whereas barbiturates increase the duration. This mechanistic distinction is a central focus of any anxiolytics and hypnotics review because it explains why barbiturates are significantly more dangerous. Unlike benzodiazepines, barbiturates can directly open the channel at high doses, leading to a lack of a safety ceiling.
How do Z-drugs like zolpidem differ from traditional benzodiazepines?
Z-drugs like zolpidem are chemically distinct from benzodiazepines but share a similar binding site. Their main advantage is selectivity for the alpha-1 subunit of the GABA-A receptor, which primarily mediates sedation. This specificity means they don’t significantly alter sleep architecture or REM cycles. Consequently, patients often experience fewer daytime side effects and less cognitive impairment compared to those taking traditional benzodiazepine hypnotics.
Why is buspirone preferred for long-term management of generalized anxiety disorder?
Buspirone is favored for long-term management because it lacks the sedative, muscle-relaxant, and anticonvulsant properties of benzodiazepines. Since it’s a 5-HT1A partial agonist and not a GABA modulator, it doesn’t carry a risk of tolerance, dependence, or withdrawal. This makes it an ideal choice for patients with a history of substance abuse or those who need to maintain full cognitive function during the day.
What happens during a benzodiazepine overdose and how is it treated?
A benzodiazepine overdose typically results in significant CNS depression, though respiratory depression is often mild unless other substances are involved. Treatment involves supportive care and the administration of Flumazenil, which is a competitive antagonist at the BZD binding site. Clinicians must verify the patient’s history first, as Flumazenil can trigger life-threatening seizures in individuals who have developed a physiological dependence on benzodiazepines.
Can barbiturates be used for anesthesia and why are they dangerous?
Barbiturates like Thiopental were traditionally used for the rapid induction of anesthesia due to their high lipid solubility. They’re dangerous because of their narrow therapeutic index and potent induction of hepatic enzymes. Because they increase the duration of chloride channel opening without a ceiling effect, they can easily progress to medullary depression. This causes fatal respiratory failure and cardiovascular collapse if the dosage isn’t meticulously controlled.
Which sedative-hypnotic drugs are safe for patients with liver disease?
Patients with impaired liver function should be prescribed the “LOT” drugs: Lorazepam, Oxazepam, and Temazepam. These specific agents are high-yield topics in an anxiolytics and hypnotics review because they bypass Phase I oxidative metabolism. Instead, they’re cleared through direct Phase II glucuronidation. This pathway remains relatively intact even in advanced cirrhosis, reducing the risk of drug accumulation and toxic sedation in hepatically compromised patients.
What is the mechanism of action for orexin receptor antagonists?
Orexin receptor antagonists work by inhibiting the body’s natural arousal system rather than inducing global CNS depression. They block the binding of orexin-A and orexin-B to OX1 and OX2 receptors in the lateral hypothalamus. By silencing these “wake” signals, medications like Suvorexant allow the brain to transition naturally into sleep. This mechanism is particularly useful for patients who struggle with an overactive wake-sleep switch.
How long does it take for buspirone to start working?
Buspirone is not an as-needed medication and typically requires 1 to 2 weeks of daily administration before the patient feels a reduction in anxiety. It can sometimes take up to 4 weeks to reach its full therapeutic potential. Healthcare providers must manage patient expectations early, explaining that the lack of immediate sedation is a trade-off for the drug’s superior safety and lack of addiction potential.