Pharmacology of Diabetes Medications Study Guide: 2026 Master Review
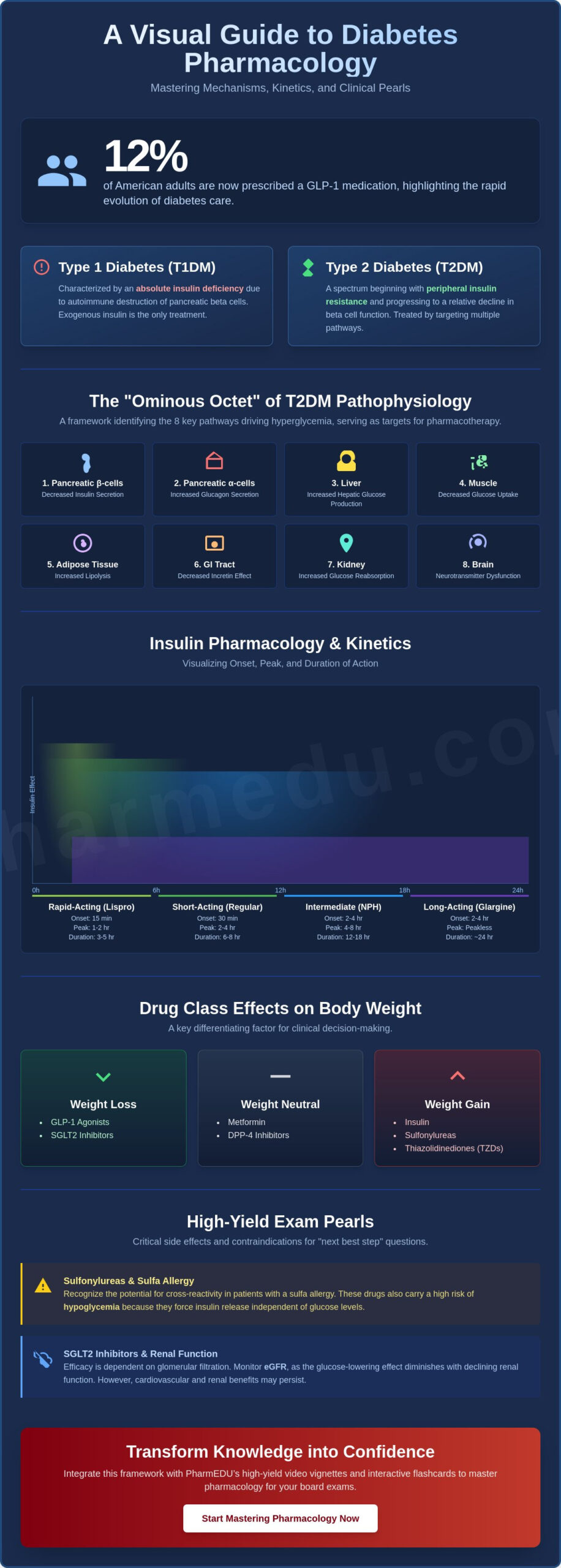
With 12% of American adults now prescribed a GLP-1 medication and the May 2026 patent expiration of Januvia fundamentally changing prescribing patterns, the complexity of endocrine pharmacology has reached a new peak. This pharmacology of diabetes medications study guide provides the high-yield framework you need to organize this vast amount of information into a logical, clinical structure.
We understand that memorizing dozens of overlapping mechanisms of action while trying to keep insulin peak times straight can make board preparation feel overwhelming. It’s difficult to feel confident when clinical vignettes hinge on specific contraindications like renal impairment or the subtle nuances of the latest 2026 ADA Standards of Care. You aren’t alone in feeling that the sheer volume of new drug approvals, from oral orforglipron to once-weekly basal insulins, makes it hard to stay current.
This master review helps you build a clear mental map of all DM medications, ensuring you can identify the “next best step” in any clinical scenario. We’ll break down the 2026 AACE management algorithms, simplify complex insulin kinetics, and provide the precise knowledge required to pass your pharmacology board exams with total confidence.
Key Takeaways
- Identify the “Ominous Octet” of physiological pathways to create a logical framework for mapping every major class of diabetes medication.
- Master the critical molecular differences and timing kinetics between rapid-acting, short-acting, and intermediate-acting insulin suspensions.
- Leverage this pharmacology of diabetes medications study guide to differentiate between weight-neutral, weight-gaining, and weight-losing drug classes for clinical vignettes.
- Recognize essential contraindications and cross-reactivity risks, such as the relationship between sulfonylureas and sulfa allergies, to excel at “next best step” questions.
- Integrate PharmEDU’s high-yield video vignettes and interactive flashcards to transform complex drug-receptor interactions into long-term clinical knowledge.
Core Pathophysiology and Pharmacological Targets in Diabetes
Mastering this pharmacology of diabetes medications study guide requires a deep understanding of why specific drugs are chosen for different patient profiles. The fundamental distinction lies in the nature of the disease. Type 1 Diabetes Mellitus (T1DM) is defined by an absolute insulin deficiency resulting from the autoimmune destruction of pancreatic beta cells. Because there’s no endogenous insulin production, exogenous insulin remains the only viable pharmacological intervention. Type 2 Diabetes Mellitus (T2DM), however, represents a spectrum. It begins with peripheral insulin resistance in the muscle and adipose tissue, eventually progressing to a relative decline in beta cell function.
To treat T2DM effectively, clinicians must address the “Ominous Octet,” a framework identifying eight distinct physiological pathways that drive hyperglycemia. These targets include the liver, where excessive glucose production occurs; the muscles, which suffer from impaired glucose uptake; and the gastrointestinal tract, where the incretin effect is often diminished. This Overview of Diabetes Medications provides a structural look at how our modern therapeutic arsenal has moved beyond the pancreas to target these diverse systems. By understanding these targets, you can logically predict which medication class will best address a patient’s specific clinical presentation.
The Mechanism of Insulin Secretion
Insulin release is a complex process centered on the ATP-sensitive potassium (K-ATP) channel within pancreatic beta cells. When blood glucose rises, its metabolism inside the cell increases the ATP-to-ADP ratio, which closes these K-ATP channels. This closure causes membrane depolarization, opening voltage-gated calcium channels and triggering insulin exocytosis. Sulfonylureas and meglitinides are potent because they bind directly to the SUR1 subunit of the K-ATP channel. They force the channel to close, bypassing the cell’s natural glucose-sensing mechanisms. This explains why these drugs carry a higher risk of hypoglycemia compared to agents that rely on the “incretin effect,” where oral glucose triggers a significantly higher insulin response than intravenous glucose due to gut-derived hormones.
Renal Glucose Reabsorption and SGLT2
The kidneys contribute to glucose homeostasis by reabsorbing nearly all filtered glucose in the proximal convoluted tubule. In healthy individuals, the renal threshold for glucose is approximately 180 mg/dL; once blood sugar exceeds this level, glucose begins to appear in the urine. SGLT2 inhibitors, often called “gliflozins,” pharmacologically lower this threshold. By blocking the sodium-glucose co-transporter 2, they promote the excretion of glucose regardless of insulin sensitivity. Because this mechanism depends on the filtration of glucose, a patient’s estimated glomerular filtration rate (eGFR) is a critical prerequisite. As renal function declines, the glucose-lowering efficacy of this class diminishes, though their cardiovascular benefits remain a cornerstone of the 2026 ADA Standards of Care.
Insulin Pharmacology: Kinetics, Onset, and Peak Times
Insulin remains the cornerstone of glycemic control for all T1DM patients and many with advanced T2DM. This pharmacology of diabetes medications study guide emphasizes that knowing the molecular logic behind insulin analogs helps you predict clinical outcomes without rote memorization. Rapid-acting analogs like Insulin Lispro incorporate specific amino acid substitutions that prevent the formation of stable hexamers. This allows for immediate dissociation into monomers and rapid absorption into the systemic circulation. In contrast, Regular insulin exists as hexamers that must dissociate before entering the bloodstream, resulting in a delayed onset and a longer duration of action.
Intermediate-acting NPH insulin is unique because it’s a suspension of insulin with protamine and zinc. This creates the characteristic cloudy appearance and requires gentle rolling before administration to ensure a homogenous mixture. While NPH bridges the gap between meals, basal insulins like Glargine and Detemir provide a steady physiological baseline. Glargine achieves its peakless, 24-hour profile by precipitating into a microprecipitate at the neutral pH of subcutaneous tissue, while Detemir uses a fatty acid side chain to bind reversibly with albumin. Understanding these mechanisms is just as vital as mastering Non-Insulin Diabetes Medications for a complete pharmacological perspective.
When mixing insulins, always remember the “clear before cloudy” rule. This prevents contaminating the rapid-acting vial with protamine from the NPH vial, which would inadvertently alter the kinetics of the fast-acting dose. Never mix long-acting basal insulins in the same syringe with other types. Their specific pH requirements for depot formation are easily compromised by other solutions, leading to unpredictable absorption rates.
High-Yield Insulin Kinetic Table
The peak time of any insulin preparation is the most clinically significant data point because it represents the window of maximum hypoglycemic risk for the patient. Rapid-acting insulins (Lispro, Aspart, Glulisine) generally follow a 15 minute onset, 1 hour peak, and 3 hour duration pattern. Short-acting Regular insulin roughly doubles these values with a 30 minute onset, 2 hour peak, and 8 hour duration. Intermediate NPH shifts the timeline significantly, reaching its peak at 8 hours and lasting up to 16 hours. For patients requiring even longer coverage, ultra-long acting Degludec forms multi-hexamers in the subcutaneous tissue, providing a half-life that exceeds 25 hours. You can drill these specific timings using Interactive Pharmacology Flashcards to ensure they’re second nature before your exam.
Clinical Pearls for Insulin Administration
Patient education must focus on site rotation to prevent lipodystrophy, a localized reaction that can lead to erratic and unreliable absorption patterns. Clinicians must also distinguish between the Somogyi Effect and the Dawn Phenomenon when reviewing morning hyperglycemia. The Somogyi Effect is a rebound response to nocturnal hypoglycemia, whereas the Dawn Phenomenon is caused by a natural early-morning surge in growth hormone and cortisol. If a patient exhibits extreme insulin resistance, U-500 insulin provides a concentrated alternative, delivering five times the potency of standard U-100 concentrations in the same volume.
Oral Antidiabetics and Non-Insulin Injectables
While insulin is essential for survival in T1DM, the management of T2DM relies heavily on oral agents and non-insulin injectables that target the underlying insulin resistance and incretin defects. This pharmacology of diabetes medications study guide focuses on the high-yield nuances that frequently appear on board exams, such as renal dosing adjustments and specific metabolic side effects. Understanding these classes requires looking beyond simple glucose lowering to the systemic benefits they provide, particularly in cardiovascular and renal health.
The “Big Three” Oral Classes: Metformin, SGLT2s, and TZDs
Metformin remains the preferred first-line agent because it effectively suppresses hepatic glucose production through AMPK activation without causing hypoglycemia or weight gain. However, its use is strictly limited by renal function. You must hold Metformin for 48 hours before and after procedures involving IV contrast dye to mitigate the risk of lactic acidosis. Long-term use also necessitates monitoring for B12 deficiency, which can mimic diabetic neuropathy. In contrast, Thiazolidinediones (TZDs) like Pioglitazone improve peripheral insulin sensitivity via PPAR-gamma activation. These carry a significant black box warning for heart failure due to fluid retention and are associated with an increased risk of bone fractures.
SGLT2 inhibitors, or the “gliflozins,” have revolutionized T2DM care by providing significant cardiovascular and renal protection. By inhibiting glucose reabsorption in the kidneys, they promote osmotic diuresis and weight loss. Clinicians must watch for unique complications such as mycotic genital infections and the rare but dangerous euglycemic diabetic ketoacidosis (DKA). In these cases, patients present with metabolic acidosis despite having relatively normal blood glucose levels, making it a critical “next best step” diagnostic challenge on exams.
Incretin Mimetics: GLP-1 and GIP Dual Agonists
The incretin system has become a primary target for both glycemic control and weight management. GLP-1 receptor agonists like Semaglutide mimic natural gut hormones to delay gastric emptying and increase satiety. The newer dual agonists, such as Tirzepatide, target both GLP-1 and Glucose-dependent Insulinotropic Polypeptide (GIP) receptors, leading to even more profound reductions in A1c and body weight. To address availability and patient-specific needs, clinicians may explore Compounded Tirzepatide as an alternative delivery method. If a patient prefers an oral option with a similar mechanism but less gastrointestinal distress, DPP-4 inhibitors (the “gliptins”) offer a weight-neutral alternative by preventing the breakdown of endogenous incretins.
Safety is paramount when prescribing these potent injectables. All GLP-1 and dual agonists are contraindicated in patients with a personal or family history of Medullary Thyroid Carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). They also carry warnings for acute pancreatitis, requiring immediate cessation if a patient presents with severe abdominal pain radiating to the back. Mastering these distinctions is a core component of any effective pharmacology of diabetes medications study guide.
Exam Strategy: Side Effects, Contraindications, and Lab Monitoring
Success on clinical exams requires moving beyond knowing what a drug does to understanding when it should never be used. This pharmacology of diabetes medications study guide highlights that board questions often focus on the “next best step” when a patient presents with a specific comorbidity. A primary differentiator in clinical vignettes is the drug’s effect on weight. You’ll need to remember that Sulfonylureas, Thiazolidinediones (TZDs), and insulin typically cause weight gain. Conversely, SGLT2 inhibitors and GLP-1 receptor agonists are favored in patients with obesity because they promote weight loss through caloric excretion and increased satiety.
Specific patient allergies and concurrent medications also dictate therapeutic choices. For example, Sulfonylureas contain a sulfonamide moiety, which traditionally suggests a risk of cross-reactivity in patients with severe sulfa allergies. Another high-yield exam pearl involves the use of non-selective Beta-Blockers. These medications can mask the adrenergic symptoms of hypoglycemia, such as tremors and tachycardia. Only diaphoresis remains as a reliable sign of low blood sugar in these patients, making it a frequent trap in clinical case studies.
Renal function is the most common limiting factor for oral antidiabetics. While we’ve discussed the mechanism of SGLT2 inhibitors, you must remember that their efficacy depends on the kidneys’ ability to filter glucose. As the eGFR drops, these drugs become less effective at lowering A1C, though they may still provide renal protection. Before your next exam, you can test your ability to spot these clinical red flags with our Pharmacology Practice Quizzes.
Black Box Warnings and Absolute Contraindications
Metformin is absolutely contraindicated in patients with an eGFR below 30 mL/min due to the significantly increased risk of lactic acidosis. For patients with Thiazolidinedione prescriptions, fluid retention is the primary deal-breaker; these drugs are strictly avoided in those with NYHA Class III or IV Heart Failure. When monitoring patients on GLP-1 receptor agonists, stay alert for signs of acute pancreatitis. Clinical vignettes will often describe a patient with severe, persistent epigastric pain that radiates to the back, which requires immediate discontinuation of the medication.
Lab Values and Diagnostic Criteria
The 2026 ADA Standards of Care generally recommend an A1C target of less than 7% for most non-pregnant adults. However, these goals are individualized, often reaching less than 8% for elderly patients or those with a history of severe hypoglycemia. For diagnosis, a Fasting Plasma Glucose (FPG) of 126 mg/dL or higher, or a 2-hour Oral Glucose Tolerance Test (OGTT) of 200 mg/dL or higher, confirms diabetes. Finally, during the management of Diabetic Ketoacidosis (DKA), monitoring potassium levels is vital. Because IV insulin therapy shifts potassium into the intracellular space, you must ensure the patient isn’t hypokalemic before starting the infusion.
Mastering Pharmacology with PharmEDU High-Yield Resources
Effective preparation for professional board exams requires more than reading a list of drug classes. It demands a structured approach that bridges the gap between physiological theory and clinical application. While this pharmacology of diabetes medications study guide has provided the foundational map, long-term retention depends on active recall and multi-modal learning. PharmEDU’s High-Yield Video Vignettes are designed to simplify complex drug-receptor interactions, such as how SGLT2 inhibitors manipulate renal thresholds or the intracellular cascade of GLP-1 receptor activation, turning abstract concepts into visual memories.
Our interactive pharmacology flashcards allow you to drill insulin peak times and drug suffixes until they become second nature. These tools aren’t just simple definition cards; they’re designed to force the mental connections needed for “next best step” clinical questions. To simulate the pressure of the NAPLEX or NCLEX, our clinical case studies replicate real-world vignettes. These scenarios challenge you to identify contraindications, like renal impairment or heart failure, in a timed environment that mirrors current national board standards. These micro-learning segments are specifically engineered for the busy 2026 healthcare student who needs to maximize every minute of study time.
From Content to Certification
Moving from content mastery to professional certification is a methodical process that requires constant self-assessment. PharmEDU’s question banks are calibrated to the specific difficulty level of national exams, ensuring there are no surprises on test day. You can track your progress across different therapeutic categories through our mobile-compliant platform, making it easy to fit high-quality study sessions into a demanding clinical schedule. If you’re looking for broader support beyond endocrine medications, explore our comprehensive pharmacology study guide for nursing students.
Start Your Pharmacology Mastery Today
Thousands of healthcare students trust PharmEDU because we prioritize high-yield information over academic fluff. We understand that your time is limited, so our resources focus on the facts and safety parameters most likely to appear on your boards. This pharmacology of diabetes medications study guide is just one part of our extensive library. You can also see our ACE Inhibitors Pharmacology Guide for more high-yield content. Don’t leave your professional future to chance. Join PharmEDU and Ace Your Exams to secure the confidence you need for clinical success.
Advance Your Clinical Expertise Today
Mastering the modern landscape of diabetes management requires a precise understanding of how physiological targets translate into successful clinical outcomes. From navigating the rapid onset of insulin analogs to identifying the cardiovascular benefits of SGLT2 inhibitors, this pharmacology of diabetes medications study guide provides the high-yield structure necessary for exam success. By focusing on the “Ominous Octet” and specific contraindications like renal thresholds, you’ve built a mental map that moves beyond simple memorization into true clinical reasoning.
Solidifying this knowledge is the final step toward certification. PharmEDU provides over 100 High-Yield Video Topics and NAPLEX and NCLEX aligned content to ensure you’re prepared for any clinical vignette. Our mobile-compliant learning platform allows you to drill these concepts whenever your schedule permits, turning downtime into productive review. You don’t have to face your board exams with uncertainty.
Master Diabetes Pharmacology with PharmEDU Subscriptions and gain the confidence required to excel in your professional journey. Your commitment to high-quality patient care starts with the mastery you achieve today. We’re here to support your growth every step of the way.
Frequently Asked Questions
Which diabetes medication is contraindicated in patients with heart failure?
Thiazolidinediones (TZDs), such as Pioglitazone and Rosiglitazone, are strictly contraindicated in patients with NYHA Class III or IV heart failure. These medications promote sodium and water reabsorption in the renal tubules, leading to fluid retention and peripheral edema. For a student using a pharmacology of diabetes medications study guide, recognizing this link is vital, as fluid overload can rapidly exacerbate underlying cardiac dysfunction.
What is the most common side effect of Metformin and how can it be mitigated?
Gastrointestinal distress, including diarrhea, nausea, and abdominal cramping, is the most frequently reported side effect of Metformin. To improve patient adherence, clinicians often recommend taking the medication with a meal or starting at a low dose and titrating slowly. Switching to an extended-release (ER) formulation also reduces these symptoms by slowing the drug’s delivery into the gastrointestinal system.
How do SGLT2 inhibitors provide cardiovascular protection?
SGLT2 inhibitors provide cardiovascular benefits by promoting osmotic diuresis and natriuresis, which reduces both preload and afterload on the heart. This class also induces a metabolic shift that improves myocardial energetics. These systemic effects help reduce the risk of hospitalization for heart failure and major adverse cardiovascular events, making them a cornerstone of modern T2DM management for high-risk patients.
Can Type 1 diabetics take oral hypoglycemic agents?
Standard clinical practice and board exams dictate that Type 1 diabetics cannot rely on oral hypoglycemic agents because they have an absolute insulin deficiency. While some clinicians explore adjunct therapies off-label, exogenous insulin remains the only life-sustaining treatment. Oral agents like Metformin or Sulfonylureas require endogenous insulin production or specific peripheral receptors that are insufficient in T1DM pathophysiology.
What are the rapid-acting insulin onset and peak times?
Rapid-acting insulins, such as Lispro, Aspart, and Glulisine, typically feature an onset of action within 15 minutes and reach their peak effect at approximately 1 hour. Because of this rapid profile, patients must administer the dose immediately before or after a meal. This timing is a critical component of any pharmacology of diabetes medications study guide, as the peak represents the period of highest hypoglycemic risk.
What is the black box warning associated with Thiazolidinediones (TZDs)?
The primary black box warning for Thiazolidinediones (TZDs) concerns the risk of causing or exacerbating congestive heart failure. Because these drugs activate PPAR-gamma receptors, they increase fluid volume, which can be dangerous for patients with compromised cardiac output. Clinicians must monitor patients closely for rapid weight gain, dyspnea, or edema and discontinue the medication if heart failure symptoms develop.
Why must Metformin be held before a procedure involving IV contrast dye?
Metformin must be held for 48 hours before and after procedures using iodinated contrast dye to prevent the development of lactic acidosis. If the contrast dye causes acute kidney injury, Metformin can accumulate to toxic levels in the blood. This accumulation interferes with mitochondrial function and leads to a life-threatening buildup of lactic acid, especially in patients with pre-existing renal impairment.
What are the signs of hypoglycemia that students should look for in exam vignettes?
Exam vignettes typically present hypoglycemia through adrenergic and neuroglycopenic symptoms. Adrenergic signs include diaphoresis, tremors, tachycardia, and palpitations, which are caused by the body’s compensatory surge of epinephrine. Neuroglycopenic symptoms manifest as the brain is deprived of glucose, appearing as confusion, irritability, or visual disturbances. Students should remember that beta-blockers can mask all these signs except for diaphoresis.