Chemotherapy Drugs Nursing Considerations: The High-Yield Guide for 2026
You don’t need to memorize the molecular mechanism of every single antineoplastic agent to be a safe, effective clinician. While the sheer volume of new targeted therapies and antibody-drug conjugates can feel overwhelming, clinical excellence isn’t about rote memorization. It’s about mastering the rigid safety protocols and the “Big Four” toxicities that protect both you and your patient. We understand the pressure of staying current, especially with the 2024 ASCO/ONS standards now requiring a fourth verification step and mandatory fertility preservation counseling before the first dose. These chemotherapy drugs nursing considerations are the difference between a high-stress shift and a confident, controlled clinical practice.
This high-yield guide provides the exact framework you need to master essential nursing interventions, safety protocols, and drug-specific toxicities for board exam success and clinical excellence. You’ll learn how to connect shifting lab values to specific drug toxicities without the usual guesswork. We’ll explore the latest 2026 standards for home administration, the move toward personalized immunotherapy, and the critical steps for managing hazardous drug exposure so you can focus on what matters most: patient care.
Key Takeaways
- Identify your legal responsibilities as the final safety link in the antineoplastic administration chain and the importance of professional certification.
- Master essential chemotherapy drugs nursing considerations by focusing on high-yield drug prototypes and their specific cellular targets.
- Differentiate between anticipatory and delayed nausea to provide timely pharmacological and psychosocial support for patients.
- Apply critical assessment skills to monitor renal function and calculate Absolute Neutrophil Counts for accurate infection risk management.
- Streamline your study process using interactive Pharmacology Practice Quizzes and clinical case studies to bridge the gap between theory and practice.
Core Principles of Cytotoxic Safety and Handling
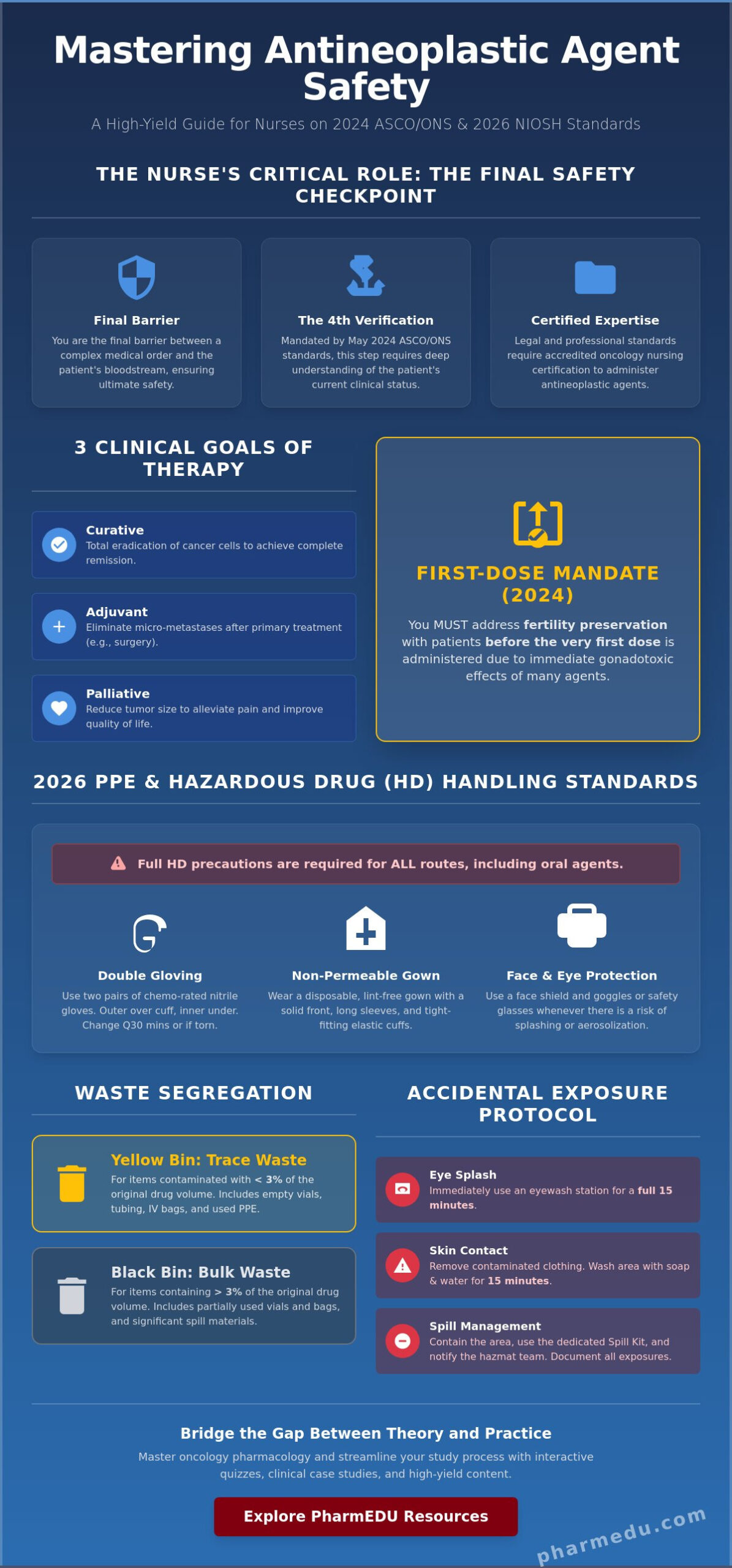
The bedside nurse functions as the ultimate safety check in the antineoplastic administration chain. While pharmacists and oncologists calculate and prepare the agents, you’re the one verifying the “Fourth Verification” step introduced in the May 2024 ASCO/ONS standards. This role requires more than just a double check of the pump settings; it demands a deep understanding of the patient’s current clinical status and the specific protocol requirements. Mastering chemotherapy drugs nursing considerations is essential for maintaining a safe environment for both the patient and the healthcare team. You’re the final barrier between a complex medical order and a patient’s bloodstream.
Antineoplastic therapy, the modern term for Chemotherapy, serves three primary clinical goals. Curative therapy aims for the total eradication of cancer cells to achieve a complete remission. Adjuvant therapy is administered after a primary treatment, like surgery, to eliminate any remaining micro-metastases. Palliative therapy focuses on reducing tumor size to alleviate pain and improve the quality of life when a cure isn’t the primary objective. Regardless of the goal, the legal and professional requirement for specialized certification is absolute. You shouldn’t administer these agents without completing an accredited oncology nursing program that covers the latest 2024 safety updates.
Hazardous drug (HD) protocols aren’t just for IV infusions. Oral antineoplastic agents carry the same risks of mutagenicity and carcinogenicity to the handler. Nurses often mistakenly handle oral tablets with standard gloves, but NIOSH standards for 2026 emphasize that all routes require full hazardous drug precautions. This includes the 2024 mandate to address fertility preservation with patients before the very first dose is administered, as many of these agents have immediate gonadotoxic effects.
2026 PPE Standards: Protecting the Provider
Protection begins with double gloving. You must use two pairs of chemotherapy-rated nitrile gloves, with the inner glove under the gown cuff and the outer glove over it. Change these every 30 minutes or immediately if they’re punctured. Use non-permeable, lint-free gowns and full face protection whenever there’s a risk of splashing. Disposal is equally critical. Use yellow bins for “Trace Chemo” waste, such as empty vials and used tubing. Reserve black bins for “Bulk Chemo” waste, which includes any container holding more than 3% of its original volume or significant spills.
Managing Accidental Exposure and Spills
If skin contact occurs, immediately remove contaminated clothing and wash the affected area with soap and water for 15 minutes. For eye splashes, use an eyewash station for a full 15 minutes. Every unit must have a dedicated “Spill Kit” containing absorbent pads, respirators, and neutralizing agents. It’s your responsibility to contain the area and notify the hazardous materials team. Document every exposure according to your institutional policy and national reporting requirements to ensure long-term health monitoring.
High-Yield Chemotherapy Drug Classes and Prototypes
Organizing chemotherapy drugs nursing considerations by drug class is the most efficient way to prepare for clinical practice and board exams. Instead of memorizing each agent in isolation, focus on how they disrupt the cell cycle. Alkylating agents, for instance, work by cross-linking DNA strands. This prevents the cell from replicating, regardless of which phase it’s in. While effective, these drugs carry a significant long-term risk of secondary malignancies, such as leukemia, which can develop years after treatment ends. Antimetabolites, however, are cell-cycle specific. They primarily disrupt the S-phase by mimicking essential nutrients, effectively “tricking” the cancer cell into using faulty building blocks for DNA synthesis.
Antitumor antibiotics are often a source of confusion for new nurses. Despite the name, these aren’t used to treat infections. They’re isolated from soil fungi and work by distorting DNA structure or inhibiting topoisomerase. Mitotic inhibitors, such as the taxanes and vinca alkaloids, target the M-phase. They interfere with microtubule formation, which is essential for cell division. If you’re struggling to keep these mechanisms straight, our Interactive Pharmacology Flashcards provide a structured way to master these toxicities through active recall.
The ‘Red Devil’ and Beyond: Prototype Drugs to Know
- Doxorubicin: Known as the “Red Devil” for its color and potency, this antitumor antibiotic is notorious for cardiotoxicity. You must verify a baseline echocardiogram and monitor the Left Ventricular Ejection Fraction (LVEF). Most patients have a strictly tracked “lifetime cumulative dose” to prevent irreversible heart failure.
- Cyclophosphamide: This alkylating agent can cause hemorrhagic cystitis. Your primary nursing action is to encourage aggressive hydration and ensure the patient receives Mesna, a uroprotective agent that neutralizes toxic metabolites in the bladder.
- Vincristine: Unlike most cytotoxic agents, vincristine is bone marrow sparing, meaning it has a low risk for myelosuppression. However, it carries a high risk for peripheral neuropathy. Monitor for “foot drop,” numbness in extremities, and severe constipation.
- Cisplatin: This is the “heavy hitter” for nephrotoxicity. You’ll often spend hours “pre-gaming” the patient with liters of IV fluids to flush the kidneys before administration.
Hormonal and Targeted Therapies
Hormonal therapies like Tamoxifen are common in breast cancer treatment. Because they block estrogen receptors, patients often experience “medical menopause,” characterized by hot flashes and an increased risk of deep vein thrombosis (DVT). When administering monoclonal antibodies (mAbs), your focus shifts to the infusion site. These agents frequently trigger hypersensitivity reactions, requiring you to have emergency medications like diphenhydramine and epinephrine at the bedside. Targeted therapy interferes with specific molecules involved in tumor growth, whereas traditional cytotoxic chemotherapy kills all rapidly dividing cells.
Managing Common Side Effects: The Nursing Process
Effective management of chemotherapy drugs nursing considerations requires a proactive approach to side effect prevention. Chemotherapy-induced nausea and vomiting (CINV) remains one of the most feared complications for patients. You must distinguish between anticipatory nausea, which is a conditioned response to the clinical environment, and delayed nausea, which peaks 24 to 48 hours after administration. Evidence-based practice now favors the use of scheduled antiemetics rather than “as needed” dosing to maintain a therapeutic window. Oral health is equally critical. Stomatitis and mucositis can lead to severe pain and secondary infections. You should implement a strict oral care protocol using soft-bristled brushes and salt-and-soda rinses. Avoid alcohol-based mouthwashes, as they dry the mucosa and exacerbate tissue breakdown.
The psychosocial impact of cancer treatment is often as taxing as the physical symptoms. Alopecia can profoundly disturb a patient’s body image and sense of self. Address this early by discussing scalp cooling options or referral to support services before hair loss begins. Additionally, many patients struggle with “Chemo Brain” and cancer-related fatigue. These aren’t just minor inconveniences; they’re debilitating symptoms that affect daily functioning. Encourage patients to use “energy banking” techniques, prioritizing essential tasks during their highest energy periods of the day.
Myelosuppression: The Most Dangerous Side Effect
Myelosuppression is the primary dose-limiting toxicity for most cytotoxic agents. You must track the “Nadir,” which is the point at which blood cell counts reach their lowest level, typically 7 to 14 days after treatment. When the Absolute Neutrophil Count (ANC) drops below 500/mm³, the patient enters a state of severe neutropenia, requiring immediate protective isolation. Thrombocytopenia also poses a significant risk. You should implement bleeding precautions when platelet counts fall below 50,000/mm³ and prepare for transfusion if they drop below 10,000 to 20,000/mm³ or if the patient becomes symptomatic.
Patient Education for Home Care
With the 2024 shift toward more at-home antineoplastic administration, patient education is vital for family safety. Instruct patients to double-flush the toilet and wash contaminated laundry separately for 48 to 72 hours post-treatment. Temperature monitoring is a non-negotiable requirement. In a neutropenic patient, a fever of 100.4°F (38.0°C) is a medical emergency that requires immediate evaluation. Modern food safety has moved away from the restrictive “Neutropenic Diet” myth. Instead, focus on rigorous food handling, such as washing all produce thoroughly and ensuring meats are cooked to safe internal temperatures, to prevent foodborne illness.
Critical Assessments, Labs, and Emergency Interventions
Mastering laboratory interpretation is where clinical knowledge transforms into patient safety. You can’t rely on the “normal” range on a lab report; you must understand how these values shift in response to specific agents. For example, calculating the Absolute Neutrophil Count (ANC) is the only reliable way to gauge infection risk. Use the formula: WBC count multiplied by the percentage of neutrophils (segs + bands). When the ANC falls below 500/mm³, the risk of life-threatening sepsis becomes acute. Similarly, renal function monitoring goes beyond a simple serum creatinine. For drugs like cisplatin, a 24-hour urine collection for creatinine clearance provides a more precise picture of the kidneys’ ability to filter cytotoxic metabolites. If you see rising BUN or ALT levels, you’re looking at early indicators of nephrotoxicity or hepatotoxicity that may require immediate dose adjustments.
Tumor Lysis Syndrome (TLS) represents a true oncologic emergency where the rapid destruction of cancer cells floods the bloodstream with intracellular contents. This results in a dangerous quartet: hyperuricemia, hyperkalemia, hyperphosphatemia, and hypocalcemia. You must monitor for cardiac arrhythmias and renal failure, often initiating aggressive hydration and allopurinol before treatment begins. To test your ability to recognize these patterns under pressure, try our Pharmacology Practice Quizzes, which feature real-world clinical scenarios.
Extravasation: Preventing Tissue Necrosis
Differentiating between vesicants and irritants is a foundational skill. Vesicants, such as doxorubicin or vincristine, can cause permanent tissue necrosis if they leak into the surrounding space. Irritants cause pain and inflammation but don’t lead to tissue sloughing. If you suspect extravasation due to swelling, pain, or a lack of blood return, your immediate actions are to stop the infusion, leave the needle or catheter in place to aspirate residual drug, and notify the oncology team according to your facility’s protocol.
Prioritization on Board Exams
Oncology prioritization often centers on the “Who do you see first?” framework. A patient with a fever or signs of anaphylaxis always takes precedence over someone with routine nausea. You must also distinguish between a mild infusion reaction (chills, flushing) and true anaphylaxis (stridor, hypotension, wheezing). When a neutropenic patient develops a cough, the nurse’s priority action is to perform a focused respiratory assessment and notify the provider immediately, as these patients often lack the inflammatory response to produce typical signs of pneumonia. These chemotherapy drugs nursing considerations ensure you’re acting on the most critical clinical data first.
Mastering Oncology Pharmacology with PharmEDU
Traditional textbooks often struggle to keep pace with the rapid evolution of oncology. With the 2024 ASCO/ONS standards fundamentally changing how we approach antineoplastic therapy, relying on a static 500-page manual isn’t just inefficient; it’s a potential safety risk. Clinical excellence requires a more agile approach to chemotherapy drugs nursing considerations. PharmEDU replaces the dense, academic jargon of traditional resources with micro-learning modules designed for the busy professional. You can master high-yield drug classes in minutes by focusing on the “Big Four” toxicities and the specific nursing actions that prevent adverse outcomes. In an era where 80% of oncologists reported prescribing new drugs or indications in the past year, your educational tools must be as dynamic as the field itself.
The power of active recall is a cornerstone of our platform. Our Interactive Pharmacology Flashcards force your brain to retrieve information about prototype toxicities, ensuring that details like doxorubicin’s lifetime dose or cisplatin’s nephrotoxicity become second nature. This method bridges the gap between classroom theory and clinical safety. It allows you to walk into a patient’s room with the confidence that you’ve mastered the latest 2026 protocols. By focusing on high-yield content, we remove the administrative burden of sorting through irrelevant data, letting you focus on what truly matters: safe patient care.
High-Yield Study Strategies for 2026
Visualizing drug mechanisms is often more effective than reading about them. Our High-Yield Video Vignettes allow you to see drug actions and nursing interventions in a clinical context. Once you’ve reviewed the material, use our Pharmacology Practice Quizzes to identify specific knowledge gaps before they impact your practice or your exam scores. We’ve designed these tools to fit into a demanding schedule, making it possible to study effectively during a break or between shifts. Explore our pharmacology study guide for nursing students for more tips on streamlining your preparation.
Join the PharmEDU Community
Our comprehensive pharmacy review is specifically engineered to help nursing students and professionals excel in a digital-first environment. We’ve seen countless success stories where micro-learning led to board exam mastery and a significant reduction in clinical errors. Our platform serves as a digital mentor, helping you navigate the complexities of chemotherapy drugs nursing considerations with precision and authority. Don’t let the complexity of modern oncology pharmacology hold back your career. Start your PharmEDU subscription today and master chemotherapy pharmacology!
Advancing Your Oncology Nursing Practice
Mastering oncology pharmacology requires more than memorizing a list of agents. It demands a structured understanding of how the 2024 ASCO/ONS safety standards and specific drug toxicities impact bedside care. By prioritizing critical assessments like the Absolute Neutrophil Count and recognizing early signs of extravasation, you protect both your patients and your professional license. These chemotherapy drugs nursing considerations are the foundation of clinical excellence in a field that evolves almost daily.
Staying current shouldn’t feel like an administrative burden. PharmEDU is used by thousands of nursing students nationwide to bridge the gap between complex theory and safe practice. With over 100 high-yield pharmacology topics and a mobile-compliant design, you can master drug prototypes wherever you are. Unlock High-Yield Oncology Flashcards & Quizzes with PharmEDU to streamline your study process and prepare for board exam success. You have the dedication to care for oncology patients; we have the tools to ensure you do it with total confidence. Keep pushing the boundaries of your clinical knowledge.
Frequently Asked Questions
What is the most important nursing consideration when administering a vesicant chemotherapy drug?
The most critical consideration is the prevention and early detection of extravasation to avoid permanent tissue necrosis. You must verify blood return before and during administration while ensuring the patency of the intravenous site. If you suspect any leakage or the patient reports pain, your first action is to stop the infusion immediately. Leaving the cannula in place to aspirate residual medication is often required by institutional protocols before the device is removed.
When is the ‘nadir’ usually reached after a chemotherapy treatment?
The nadir, which is the point where blood cell counts reach their lowest level, typically occurs 7 to 14 days after a treatment session. This period represents the highest risk for infection and bleeding due to bone marrow suppression. Nurses must monitor the Absolute Neutrophil Count closely during this window and educate patients on recognizing early signs of fever or unusual bruising. Timing can vary slightly depending on the specific cytotoxic agent used.
What are the specific PPE requirements for nurses handling cytotoxic drugs in 2026?
Current 2026 standards require double gloving with chemotherapy-rated nitrile gloves and the use of non-permeable, lint-free gowns with long sleeves and tight cuffs. You must also wear a face shield and a respirator if there’s any risk of aerosolization or splashing during administration. These chemotherapy drugs nursing considerations for safety protect the clinician from chronic hazardous drug exposure, which is linked to mutagenic and carcinogenic risks over time.
How do you calculate the Absolute Neutrophil Count (ANC) and why does it matter?
You calculate the Absolute Neutrophil Count (ANC) by multiplying the total white blood cell (WBC) count by the percentage of neutrophils, which includes the sum of segmented neutrophils and bands. This value is the gold standard for determining a patient’s actual risk for life-threatening infection. An ANC below 500/mm³ indicates severe neutropenia, necessitating immediate protective isolation and the initiation of neutropenic precautions to prevent the development of sepsis.
What is the difference between cell-cycle specific and cell-cycle non-specific drugs?
Cell-cycle specific drugs, such as antimetabolites or mitotic inhibitors, are only effective when the cancer cell is in a particular phase of division like the S-phase or M-phase. In contrast, cell-cycle non-specific agents, including alkylating agents, can damage DNA and kill cells regardless of their current phase. Understanding this difference helps nurses anticipate the timing of side effects and the rationale behind specific combination therapy protocols used in oncology.
What should a nurse do immediately if a chemotherapy spill occurs?
If a chemotherapy spill occurs, your immediate priority is to contain the area and prevent further exposure to patients or staff. You should block off the site, notify the hazardous materials team, and use a specialized “Spill Kit” to manage the cleanup. Never attempt to clean a cytotoxic spill with standard janitorial supplies. Proper documentation of the event is required by institutional safety policies to ensure long-term health monitoring for all exposed individuals.
Why is Doxorubicin often referred to as the ‘Red Devil’ in nursing pharmacology?
Doxorubicin is frequently called the “Red Devil” because of its distinct bright red color and its high potential for severe toxicities, particularly irreversible cardiotoxicity. The medication can cause permanent damage to the heart muscle, leading to heart failure if cumulative lifetime doses are exceeded. Nurses must verify baseline cardiac function through an echocardiogram and monitor the patient’s ejection fraction throughout the duration of the treatment to ensure safety.
What are the signs of Tumor Lysis Syndrome that a nurse should monitor for?
Nurses must monitor for a specific quartet of electrolyte imbalances: hyperkalemia, hyperuricemia, hyperphosphatemia, and hypocalcemia. These shifts can lead to cardiac arrhythmias, muscle cramps, and acute renal failure as the kidneys struggle to filter the debris from rapidly dying cancer cells. Early clinical signs include decreased urine output, lethargy, and heart palpitations. These chemotherapy drugs nursing considerations for emergencies are vital for preventing rapid patient decline during initial treatment phases.