Propofol Pharmacology: The High-Yield Guide for Healthcare Students (2026)
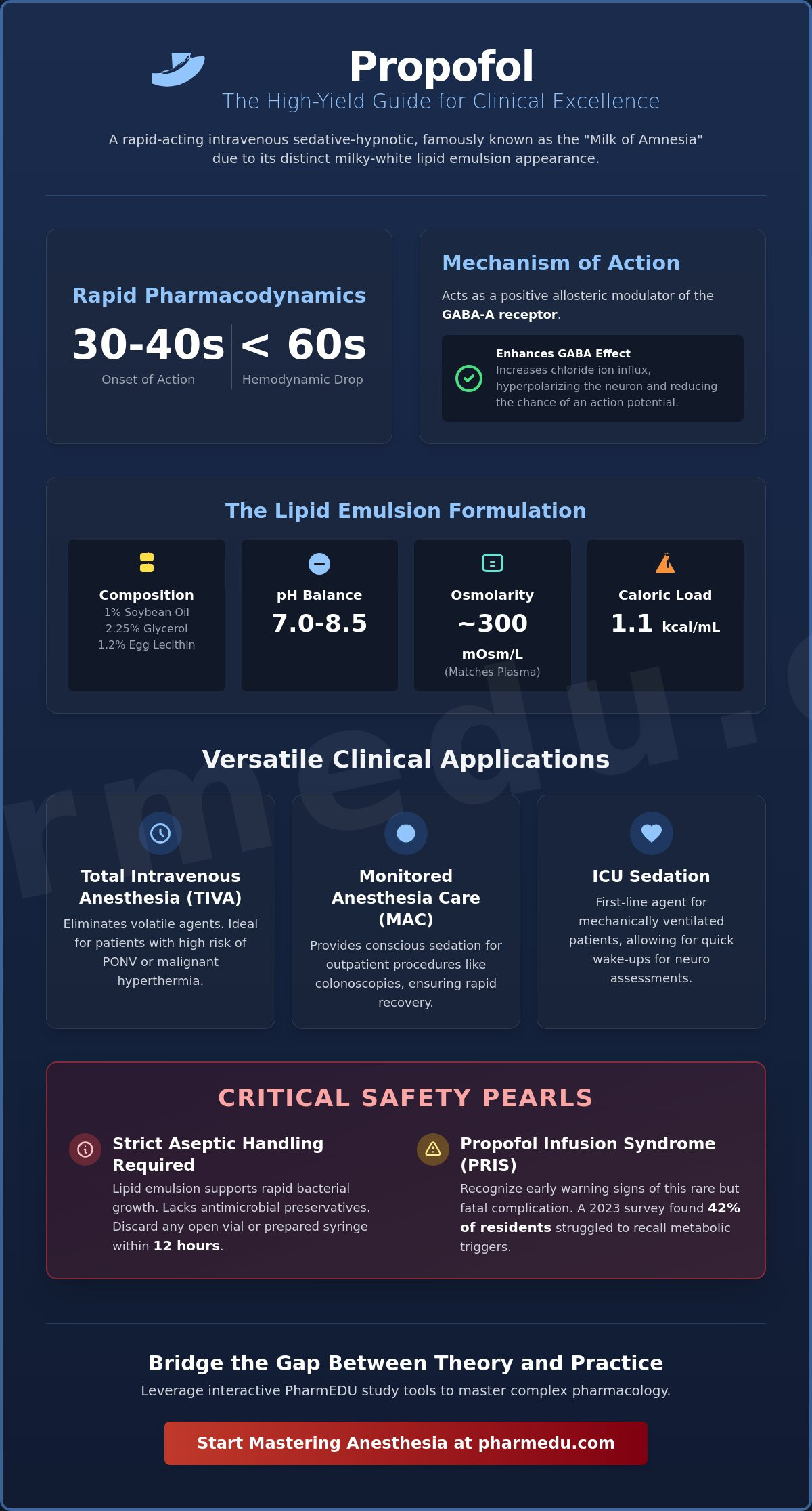
Administering an incorrect bolus of propofol can trigger a profound drop in systemic vascular resistance within 60 seconds, making it one of the most powerful yet unforgiving tools in your clinical arsenal. You’ve likely spent hours staring at the distinctive milky white emulsion in the ICU, wondering if you’ll remember the exact contraindications during a high-pressure code. A 2023 survey of medical residents found that 42% of students struggled to recall the specific metabolic triggers for PRIS during clinical rounds. It’s common to feel frustrated by dense textbooks that fail to distinguish this sedative from other induction agents with similar profiles.
I’ve designed this 2026 high-yield guide to bridge the gap between academic theory and the fast-paced reality of the operating room. You’ll master the essential GABA-A receptor mechanisms, clinical indications, and the critical safety pearls needed to excel in your rotations. We’ll break down the 2024 updated guidelines for ICU sedation protocols and provide a clear framework to identify Propofol Infusion Syndrome symptoms before they escalate. This roadmap ensures you understand lipid emulsion safety and possess the knowledge required to pass your exams with precision.
Key Takeaways
- Understand the unique chemical properties and GABA-ergic mechanism of action that define propofol as the gold standard for rapid-onset sedation.
- Differentiate between the clinical applications of TIVA and MAC to optimize patient outcomes during surgical and outpatient procedures.
- Identify critical safety pearls, including how to manage hemodynamic changes and recognize the early warning signs of PRIS.
- Decode the three-compartment pharmacokinetic model to understand why this agent allows for such rapid emergence and predictable recovery.
- Leverage interactive PharmEDU study tools to bridge the gap between complex pharmacological theory and high-yield clinical practice.
What is Propofol? Mechanism of Action and Chemical Properties
Propofol stands as a cornerstone of modern anesthesiology, functioning as a short-acting, intravenous sedative-hypnotic agent. Often called the “Milk of Amnesia” by clinicians and students alike, its nickname stems from its distinct white, opaque appearance. This visual characteristic is the result of its formulation as a soybean-oil-based emulsion, which is necessary because the drug itself is highly insoluble in water. In the clinical landscape of 2026, it remains the gold standard for the induction and maintenance of general anesthesia. What is Propofol? It’s a compound that provides rapid loss of consciousness, typically within 30 to 40 seconds of administration, followed by a quick recovery period that makes it ideal for outpatient procedures and intensive care sedation.
The GABA-A Receptor Interaction
The primary sedative effects of propofol occur through its interaction with the gamma-aminobutyric acid (GABA) system, the brain’s main inhibitory network. It acts as a positive allosteric modulator of the GABA-A receptor. When the drug binds to these receptors, it enhances the inhibitory effect of the neurotransmitter, leading to an increased influx of chloride ions into the postsynaptic neuron. This process results in hyperpolarization of the neuronal membrane, which significantly reduces the likelihood of an action potential firing.
While other sedatives like benzodiazepines and barbiturates also target the GABA-A receptor, propofol is distinct. It binds to a specific site on the beta-subunit of the receptor, different from the binding pockets used by other classes. At higher concentrations, propofol can even directly activate the GABA-A receptor in the absence of GABA, a property that contributes to its potent anesthetic depth. This mechanism ensures a predictable and dose-dependent transition from light sedation to deep surgical anesthesia.
Physical Characteristics and the Lipid Vehicle
Because propofol is highly lipophilic, it requires a specialized lipid vehicle for safe intravenous delivery. The standard formulation consists of a 1% soybean oil, 2.25% glycerol, and 1.2% purified egg lecithin emulsion. These components create a stable environment for the active molecule while ensuring compatibility with human blood. The preparation is carefully calibrated to meet physiological requirements for patient safety.
- pH Balance: The emulsion is formulated to maintain a pH between 7.0 and 8.5.
- Osmolarity: To prevent venous irritation, the solution is kept near an osmolarity of 300 mOsm/L, matching human plasma.
- Lipid Content: The 1% concentration provides approximately 1.1 kcal/mL, which must be factored into the nutritional management of patients on long-term infusions.
A critical safety factor for healthcare providers is the lack of traditional antimicrobial preservatives in most propofol formulations. The lipid-rich environment is highly susceptible to bacterial growth, including Staphylococcus aureus and Candida albicans. Consequently, strict aseptic handling is a non-negotiable requirement in every clinical setting. Current 2026 protocols dictate that any opened vial or prepared syringe must be discarded within 12 hours of being spiked or drawn to prevent the risk of healthcare-associated infections.
Clinical Indications: Anesthesia, Sedation, and Beyond
Propofol serves as the backbone of modern anesthetic practice. Its versatility allows providers to use it for Total Intravenous Anesthesia (TIVA), which eliminates the need for volatile inhalational agents. This approach is particularly beneficial for patients with a high risk of postoperative nausea or those with a family history of malignant hyperthermia. During Monitored Anesthesia Care (MAC), low-dose infusions provide comfortable sedation for outpatient procedures like colonoscopies, where a rapid return to baseline mental status is a priority.
In the Intensive Care Unit, propofol is a first-line agent for sedating mechanically ventilated patients. Its short context-sensitive half-life ensures that even after a 48-hour infusion, patients can wake up quickly for neurological assessments or weaning trials. Clinicians also utilize its potent GABA-ergic properties to treat refractory status epilepticus when traditional anticonvulsants fail. Interestingly, sub-hypnotic doses of 10 to 20 mg can effectively manage refractory nausea, making it a multi-functional tool in the perioperative setting.
Grasping the nuances of Propofol’s mechanism of action is vital for anyone managing high-acuity patients. For healthcare professionals looking to refine their clinical skills and stay current with evidence-based protocols, engaging with structured professional development resources can bridge the gap between textbook theory and bedside practice.
Induction vs. Maintenance Dosing
The drug’s high lipophilicity allows it to cross the blood-brain barrier almost instantly. Patients usually lose consciousness within 30 to 40 seconds of a standard induction bolus, typically dosed at 1.5 to 2.5 mg/kg. For maintenance, clinicians titrate a continuous infusion to reach a steady state of anesthesia. While surgical maintenance might require 100 to 200 mcg/kg/min, ICU sedation typically starts much lower, often between 5 and 50 mcg/kg/min. This careful titration is critical to prevent the accumulation of the lipid emulsion vehicle and minimize the risk of metabolic complications.
Propofol vs. Etomidate and Ketamine
Choosing the right induction agent depends entirely on the patient’s hemodynamic status. Propofol causes significant vasodilation and myocardial depression, often dropping mean arterial pressure by 15% to 25%. In cases of severe shock or cardiac instability, etomidate is often the preferred choice due to its hemodynamic neutrality. Unlike ketamine, which provides profound analgesia and sympathetic stimulation, propofol lacks any inherent pain-relieving properties. You’ve got to pair it with an analgesic if the procedure involves painful stimuli. However, propofol remains superior for neurosurgical cases because it effectively lowers intracranial pressure (ICP) and reduces cerebral oxygen consumption, protecting the brain during delicate operations.
Critical Safety: Side Effects, Contraindications, and PRIS
Safe administration of propofol requires constant vigilance because its therapeutic window is narrow. The most frequent acute side effects involve the cardiovascular and respiratory systems. Clinicians typically observe a dose-dependent decrease in systemic vascular resistance and myocardial contractility, which often leads to significant hypotension. Simultaneously, propofol acts as a potent respiratory depressant. Apnea occurs in up to 30% of patients during induction, necessitating immediate airway management capabilities. According to the DEA Drug & Chemical Evaluation, the drug’s rapid onset and short duration of action make it a preferred choice, yet these same characteristics demand continuous hemodynamic monitoring.
The “propofol sting” or intense pain on injection remains a common clinical hurdle. Roughly 70% of patients report discomfort when the drug is administered into small peripheral veins. To mitigate this, practitioners often pre-treat the site with 10 to 40 mg of lidocaine or mix the lidocaine directly into the propofol syringe. Beyond immediate administration, long-term infusions carry metabolic risks. Because the drug is formulated in a 10% lipid emulsion, it provides 1.1 kcal/mL. Healthcare teams must monitor serum triglyceride levels every 48 hours for patients receiving prolonged sedation to prevent hyperlipidemia and pancreatitis.
Absolute contraindications are straightforward but critical. Patients with a known hypersensitivity to the drug or any component of its vehicle must not receive it. This includes the lipid emulsion itself, which consists of soybean oil, glycerol, and egg lecithin.
Propofol Infusion Syndrome (PRIS)
PRIS is a rare but frequently fatal metabolic derangement associated with high-dose infusions exceeding 4 mg/kg/hr for more than 48 hours. The hallmark signs include refractory bradycardia leading to heart failure, severe metabolic acidosis, rhabdomyolysis, and hyperkalemia. The underlying mechanism involves the inhibition of mitochondrial fatty acid oxidation and the disruption of the electron transport chain. This failure of cellular metabolism creates a massive energy deficit, particularly in cardiac and skeletal muscle tissues. Early recognition and immediate cessation of the infusion are the only effective management strategies.
Egg and Soy Myths vs. Reality
The 2026 clinical consensus has clarified long-standing confusion regarding egg and soy allergies. Most patients with these allergies can safely receive propofol. The lipid emulsion uses highly purified egg lecithin, which is derived from the yolk and lacks the ovalbumin proteins that trigger most egg allergies. Similarly, the soybean oil used is highly refined and stripped of the proteins responsible for allergic reactions. While caution is warranted in patients with a history of anaphylaxis to these specific foods, the risk is statistically negligible for the majority.
Pharmacokinetics and Board Exam Study Pearls
Understanding how the body handles this anesthetic is essential for passing board exams and ensuring patient safety in the ICU or OR. It follows a three-compartment model. Think of this as a series of rooms. The first room, the central compartment, includes the blood and highly perfused organs like the brain and heart. The drug enters here immediately, explaining the 30 to 45-second onset of action. The second room is the lean muscle, and the third is the deep fat stores.
Recovery happens because the drug quickly redistributes from the brain back into the blood and other tissues. Unlike thiopental, propofol has a short context-sensitive half-life. Even after a 6-hour infusion, the plasma concentration drops by 50% within approximately 10 minutes. This rapid clearance means patients wake up clear-headed without the lingering hangover typical of benzodiazepines or older barbiturates.
Metabolism occurs primarily in the liver through glucuronidation to water-soluble conjugates. These metabolites are then cleared through renal excretion. Data suggests that clearance actually exceeds hepatic blood flow, which points to extrahepatic metabolism occurring in the lungs. This high clearance rate is why the drug doesn’t accumulate significantly in most patients, allowing for predictable offset times.
High-Yield NAPLEX and NCLEX Facts
For students preparing for licensing exams, the lipid emulsion delivery system is a frequent testing point. The drug is formulated in a 10% soybean oil emulsion, providing 1.1 kcal/mL. You must factor this into a patient’s total daily caloric intake to prevent overfeeding and hypertriglyceridemia. Because this lipid base is a perfect medium for bacteria, the CDC and ASPEN guidelines require changing the infusion tubing every 12 hours.
Use the P-R-O-P mnemonic to remember key clinical considerations:
- P: Pain on injection (mitigate with lidocaine or large veins).
- R: Rare Propofol Infusion Syndrome (PRIS) with high doses over 48 hours.
- O: Out of it quickly (rapid redistribution and clearance).
- P: Pressure drop (significant risk of hypotension).
Pharmacology for Healthcare Students: Distribution and Clearance
The volume of distribution (Vd) is a critical concept when dosing for different body habitus. Since propofol is highly lipophilic, it easily crosses the blood-brain barrier. In patients with obesity, the Vd for the third compartment increases significantly. However, since the initial effect is driven by the central compartment, we usually dose based on lean body mass for induction to avoid profound cardiovascular collapse.
To master these concepts, check out our comprehensive guide to pharmacology, which breaks down Vd and clearance for all major drug classes. Understanding these variables ensures you can adjust dosing for varied patient populations in clinical practice.
Mastering Anesthesia with PharmEDU’s High-Yield Curriculum
Mastering the clinical application of propofol requires a transition from passive reading to active recall. PharmEDU’s curriculum is designed to facilitate this shift through high-yield video vignettes that dissect general anesthetics into actionable clinical pearls. These videos don’t just list side effects; they simulate the fast-paced environment of the ICU and operating room where every second counts. By watching these expert-led sessions, you’ll see exactly how theory translates into bedside practice.
To ensure long-term retention of critical safety data, our platform utilizes interactive flashcards specifically engineered for memorizing Propofol Related Infusion Syndrome (PRIS) markers and weight-based dosing calculations. While Wikipedia provides a surface-level overview, it lacks the peer-reviewed accuracy required for high-stakes medical environments. Pharmacy students will find particular value in our NAPLEX prep course, which integrates pharmacology with real-world therapeutic management to prepare you for the 2026 boards.
- Interactive Flashcards: Master dosing math and PRIS recognition in under 10 minutes a day.
- Clinical Vignettes: Learn the nuances of sedation-agitation scales and infusion protocols through visual storytelling.
- Vetted Content: Every module is reviewed by board-certified specialists to meet 2026 clinical standards.
Why Micro-Learning Beats Traditional Textbooks
Traditional textbooks often fall short during busy clinical rotations. PharmEDU’s 5-minute high-yield videos allow you to review sedation protocols between patient rounds. This micro-learning approach aligns perfectly with our nursing pharmacology study guides, ensuring that the entire care team speaks the same clinical language. Our 2026 updates include the latest consensus guidelines on lipid emulsion monitoring and propofol titration, keeping your knowledge current and your patients safe. It’s a method that respects your time while maximizing your professional growth.
Start Your Professional Journey Today
Transitioning from a student to a certified healthcare professional is a rigorous process. PharmEDU acts as your digital mentor, providing the structure needed to excel in board exams and daily practice. We remove the administrative burden of finding reliable study materials by offering a centralized, accredited hub for all your learning needs. Whether you’re looking for an individual subscription or an institutional platform for your entire cohort, we offer the tools to bridge the gap between theory and practice.
Join thousands of successful healthcare professionals who have streamlined their education. Access our high-yield quiz today or sign up for a free trial to experience the PharmEDU difference firsthand. Your professional development shouldn’t be left to chance; choose the platform that prioritizes your clinical success and long-term career security.
Advancing Your Clinical Mastery of Intravenous Sedation
Mastering propofol pharmacology requires more than memorizing standard doses. It demands a deep understanding of rapid redistribution kinetics and the critical monitoring required to prevent Propofol Infusion Syndrome. By focusing on the drug’s specific interaction with GABA-A receptors and its significant hemodynamic impact, you’re building a reliable foundation for safe clinical practice through 2026. This guide reviewed the essential study pearls you’ll encounter on high-stakes exams and during real-world patient care in the operating room.
Standard textbooks often feel overwhelming when you’re balancing demanding clinical rotations. PharmEDU simplifies this learning process with mobile-compliant micro-learning modules designed for students who prioritize efficiency. Our platform features over 100 high-yield pharmacology topics and is already utilized by top-tier nursing and pharmacy schools to ensure student success. You’ll gain immediate access to structured, accredited content that transforms mandatory study time into genuine professional growth. It’s the most effective way to stay current with evolving medical standards while managing a busy schedule.
Master Propofol and Ace Your Boards with PharmEDU
Your journey toward becoming a precise and confident healthcare provider is a significant undertaking. We’re here to ensure every minute you spend studying delivers the maximum results for your future career.
Frequently Asked Questions
Is propofol an analgesic or just a sedative?
Propofol acts exclusively as a sedative-hypnotic agent and doesn’t provide any intrinsic pain relief. While it effectively induces unconsciousness by modulating GABA-A receptors, it can’t block nociceptive signals during surgery. Clinicians must co-administer opioids like fentanyl or use local anesthetics to manage the patient’s pain. Relying on this agent alone for painful procedures leads to dangerous sympathetic surges and increased heart rates.
Can propofol be used in patients with a severe egg allergy?
Most patients with egg allergies can safely receive propofol because the lipid emulsion uses highly purified egg lecithin rather than the proteins found in egg whites. The American Academy of Allergy, Asthma & Immunology notes that true allergic reactions to the emulsion are extremely rare. If a patient has a documented history of anaphylaxis specifically to egg yolk, providers often choose alternative induction agents like etomidate to maintain safety.
How much caloric value does propofol emulsion provide for ICU patients?
Propofol provides 1.1 kcal for every milliliter of the standard 1% emulsion, which comes from its 10% soybean oil base. ICU dietitians must track these lipid calories when calculating a patient’s total daily nutritional intake. If a patient receives an infusion at 20 mL per hour, they’re consuming 528 extra calories every day. Ignoring this source can lead to overfeeding and metabolic issues like hypertriglyceridemia.
What happens if propofol is infused for longer than 48 hours?
Infusing propofol for longer than 48 hours at doses above 4 mg/kg/hr significantly increases the risk of Propofol Infusion Syndrome. This condition is often fatal and causes severe metabolic acidosis, rhabdomyolysis, and kidney failure. Medical teams should monitor serum triglyceride levels and arterial blood gases every 24 hours during long-term sedation. Switching to a different sedative after two days helps prevent these dangerous metabolic complications.
Is propofol safe for use in pediatric patients for anesthesia induction?
Propofol is safe and FDA-approved for anesthesia induction in children older than 2 months of age. It’s a popular choice for pediatric cases because it ensures a smooth transition to sleep and reduces postoperative vomiting. However, it’s strictly contraindicated for long-term sedation in pediatric intensive care units. This restriction exists because children have a higher risk of developing fatal metabolic acidosis during prolonged infusions.
What is the most common cause of death in Propofol Infusion Syndrome (PRIS)?
Refractory bradycardia that progresses to asystole is the primary cause of death in patients suffering from Propofol Infusion Syndrome. This heart failure is typically resistant to standard ACLS medications and follows specific ECG changes similar to Brugada syndrome. Data shows that mortality rates for PRIS range from 18% to 32% depending on the speed of diagnosis. Early detection of rising lactate levels is the best way to prevent cardiac collapse.
How quickly does a patient typically wake up after stopping a propofol infusion?
Patients usually regain consciousness within 8 to 10 minutes after the clinician stops the propofol infusion. This rapid recovery happens because the drug quickly redistributes from the brain into other tissues like muscle and fat. Even after several hours of surgery, most patients can follow simple commands within 15 minutes of reaching the recovery room. Its short context-sensitive half-life makes it the ideal choice for modern outpatient procedures.