

ACE Inhibitors Pharmacology: The High-Yield Guide for Healthcare Students (2026)
According to 2023 clinical data, nearly 25% of patients prescribed ace inhibitors for hypertension will eventually report a persistent, non-productive cough. It’s a statistic that highlights why a deep understanding of the biochemical nuances of these drugs is vital for your clinical success. You likely feel the pressure of memorizing dozens of “-pril” medications while trying to map out the complex feedback loops of the RAAS pathway. It’s easy to get lost in the sea of contraindications and electrolyte shifts during a timed 60-minute practice exam when every second counts.
This comprehensive guide provides the clarity you need by distilling complex pharmacology into high-yield, actionable insights. You’ll master the exact mechanism of action, learn to differentiate these agents from ARBs with clinical precision, and build the confidence required to tackle 2026 board questions. We’re going to analyze the essential biochemistry, explore primary clinical indications, and highlight the specific side effects that examiners prioritize in modern medical assessments.
Key Takeaways
- Deepen your understanding of the RAAS pathway to master how ace inhibitors regulate blood pressure through enzyme inhibition in the lungs.
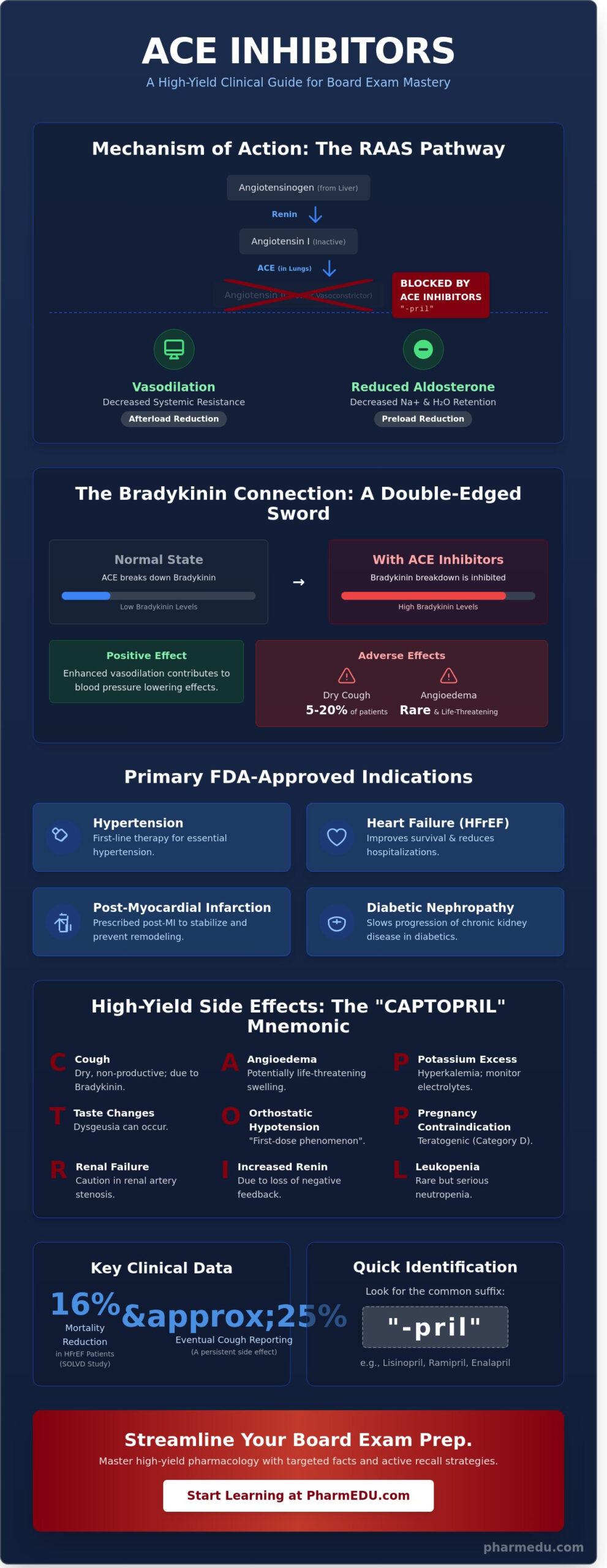
- Quickly identify this drug class using the “-pril” suffix and learn the primary FDA-approved indications for clinical practice.
- Utilize the “CAPTOPRIL” mnemonic to memorize high-yield side effects, ranging from common cough to life-threatening angioedema.
- Identify essential laboratory parameters and clinical red flags, such as the first-dose phenomenon, to ensure safe patient monitoring.
- Streamline your board exam preparation with targeted facts and active recall strategies designed for NAPLEX and USMLE success.
Understanding the RAAS Pathway and ACE Mechanism of Action
The Renin-Angiotensin-Aldosterone System (RAAS) serves as the primary endocrine regulator of systemic blood pressure and fluid homeostasis. This complex feedback loop begins when the kidneys detect low perfusion or decreased sodium delivery to the macula densa, triggering the release of renin. Renin then cleaves angiotensinogen into angiotensin I, a relatively inactive decapeptide. The most critical transformation occurs within the pulmonary vascular endothelium. Here, the Angiotensin-Converting Enzyme (ACE) facilitates the conversion of angiotensin I into angiotensin II, a potent octapeptide vasoconstrictor. By utilizing ACE inhibitors, clinicians can effectively interrupt this cascade. This pharmacological intervention prevents the formation of angiotensin II, which directly leads to systemic arterial vasodilation and a significant reduction in the secretion of aldosterone from the adrenal cortex.
The Role of Bradykinin in ACE Inhibition
ACE isn’t just responsible for activating angiotensin; it’s also the primary enzyme for degrading bradykinin within the kinin-kallikrein system. Bradykinin acts as a potent inflammatory mediator and vasodilator. When a patient starts taking ace inhibitors, the breakdown of bradykinin is inhibited, leading to its accumulation in various tissues. While this buildup enhances the drug’s blood pressure-lowering effects, it’s also the culprit behind specific adverse reactions. High concentrations of bradykinin in the upper respiratory tract can sensitize sensory neurons and trigger a dry, non-productive cough. Clinical data indicates this side effect occurs in 5% to 20% of patients. In more severe, though rarer, instances, this accumulation can lead to life-threatening angioedema, necessitating immediate cessation of the medication.
Hemodynamic Effects: Preload and Afterload
The clinical utility of these agents stems from their dual impact on cardiac loading conditions, which improves overall organ perfusion. They don’t just lower numbers on a monitor; they fundamentally change how the heart functions under stress.
- Afterload Reduction: By preventing angiotensin II-mediated vasoconstriction, these drugs lower systemic arterial resistance. This reduction in afterload makes it easier for the left ventricle to eject blood, which is vital for patients with reduced ejection fractions.
- Preload Reduction: Lower aldosterone levels lead to decreased sodium and water retention in the distal tubules. This promotes diuresis, reducing total blood volume and the pressure exerted on the heart walls before contraction.
The net result is a substantial decrease in cardiac workload and myocardial oxygen demand. Unlike direct-acting vasodilators, these agents typically don’t cause reflex tachycardia because they simultaneously blunt sympathetic activity. This balanced hemodynamic profile explains why they remain a first-line therapy for hypertension and chronic heart failure in 2026 guidelines. They provide a protective environment that prevents the pathological remodeling of cardiac tissue over time.
Clinical Indications: When and Why ACE Inhibitors are Prescribed
Identifying ace inhibitors in a clinical setting is straightforward once you recognize the common suffix “-pril.” Medications like lisinopril, ramipril, and enalapril are staples in cardiovascular medicine. Healthcare students must master these because they’re frequently the first choice for managing chronic conditions. According to this clinical overview of ACE Inhibitors, their utility spans from routine blood pressure control to complex post-infarction care. These agents aren’t just for lowering numbers; they’re prescribed to alter the course of disease progression.
The primary FDA-approved indications include:
- Essential Hypertension: Often used as first-line therapy, especially in patients with co-morbidities.
- Heart Failure with Reduced Ejection Fraction (HFrEF): Used to improve survival and reduce hospitalizations.
- Post-Myocardial Infarction: Prescribed within 24 hours of an acute MI to stabilize the patient.
- Diabetic Nephropathy: Utilized to slow the progression of chronic kidney disease.
Hypertension and Heart Failure Management
These agents are first-line therapy for HFrEF because they significantly reduce mortality and hospitalization rates. Clinical data, such as the SOLVD study, demonstrated a 16% reduction in mortality for heart failure patients using enalapril. A primary reason for this success is their ability to inhibit “cardiac remodeling.” This process involves the heart muscle thickening or stretching pathologically after an injury. By blocking Angiotensin II, ace inhibitors prevent these structural changes, preserving pump function over the long term. While they’re comparable to thiazide diuretics for uncomplicated hypertension, their survival benefit makes them superior for patients with underlying cardiac structural damage.
Diabetic Nephropathy and Renal Protection
In the kidneys, these drugs provide a unique protective effect by dilating the efferent arteriole. This specific vasodilation reduces intraglomerular pressure, which slows the progression of albuminuria and protein loss. It’s a critical intervention for diabetic patients where high pressure often leads to end-stage renal disease. Students often encounter the “renal paradox” during clinical rotations. While these drugs protect the kidneys long-term, they can cause an acute rise in serum creatinine by up to 30% within the first week of therapy. This isn’t necessarily a sign of toxicity; it’s a hemodynamic consequence of reduced filtration pressure. If you’re looking to deepen your clinical reasoning skills, exploring our accredited pharmacology modules can provide the practical edge needed for professional exams. Transitioning from acute post-MI stabilization to life-long maintenance requires careful monitoring of these renal parameters to ensure the benefit outweighs the risks.
High-Yield Side Effects and Clinical Red Flags
Understanding the side effect profile of ace inhibitors is vital for both clinical safety and exam performance. While most patients tolerate these medications well, roughly 20% of individuals may experience adverse reactions that necessitate a change in therapy. To help healthcare students memorize these effects, the mnemonic CAPTOPRIL serves as a reliable framework: Cough, Angioedema, Potassium (hyperkalemia), Taste changes (dysgeusia), Orthostatic hypotension, Pregnancy contraindication, Renal artery stenosis, Indomethacin interaction, and Leukopenia.
Hyperkalemia represents one of the most common biochemical risks associated with this drug class. When we block the conversion of Angiotensin I to Angiotensin II, we simultaneously reduce the secretion of aldosterone from the adrenal cortex. As detailed in the NIH Guide to ACE Inhibitors, this mechanism leads to systemic potassium retention because aldosterone’s primary role is to promote potassium excretion in the distal tubule. Clinicians must monitor serum potassium levels closely, particularly in patients with chronic kidney disease or those taking potassium-sparing diuretics. If potassium levels exceed 5.5 mEq/L, the medication often requires discontinuation to prevent cardiac arrhythmias.
The ACE Cough and Angioedema
A dry, non-productive cough affects between 5% and 20% of patients. This happens because the ACE enzyme normally breaks down bradykinin and substance P; when inhibited, these inflammatory mediators accumulate in the respiratory tract. If the cough becomes intolerable, the standard clinical response is to switch the patient to an Angiotensin II Receptor Blocker (ARB). Unlike the benign cough, angioedema is a medical emergency occurring in roughly 0.1% to 0.7% of users. It presents as rapid, painless swelling of the lips, tongue, and glottis. Airway management is the absolute priority in these cases, and the patient must never receive ace inhibitors again.
Teratogenicity and Pregnancy Contraindications
ACE inhibitors are strictly contraindicated during pregnancy because they are known human teratogens. Exposure during the second and third trimesters carries a high risk of fetal renal dysgenesis, skull hypoplasia, and oligohydramnios. These complications often stem from decreased fetal urine output, which is essential for maintaining amniotic fluid levels. For pregnant patients requiring blood pressure management, clinicians typically transition to safer alternatives such as Labetalol, Methyldopa, or Nifedipine to ensure both maternal and fetal safety. Maintaining professional vigilance regarding a patient’s reproductive status is a non-negotiable aspect of safe prescribing.
Drug Interactions and Clinical Monitoring
Safe administration of ace inhibitors requires a proactive approach to patient monitoring and drug-drug interactions. One of the primary concerns during initiation is the first-dose phenomenon. This characterized by a sudden, significant drop in blood pressure, which affects approximately 10 to 15% of patients, especially those already taking loop diuretics. To minimize the risk of orthostatic hypotension and syncope, clinicians often recommend that the patient takes their first dose at bedtime. If the patient is severely volume-depleted, consider withholding diuretics for 24 to 48 hours before starting therapy.
Pharmacological antagonism is another critical factor. Non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen significantly reduce the antihypertensive efficacy of these medications. NSAIDs inhibit prostaglandin synthesis, which normally helps maintain renal blood flow through afferent arteriole vasodilation. When the vasodilatory effect of ace inhibitors on the efferent arteriole is combined with NSAID-induced afferent constriction, the glomerular filtration rate (GFR) can plummet. This “triple whammy” effect, especially when a diuretic is added, increases the risk of acute kidney injury by nearly 31% in high-risk populations.
Potassium and Creatinine Monitoring
Clinicians must order baseline and follow-up renal function panels. A rise in serum creatinine is expected because the drug reduces intraglomerular pressure. An increase of up to 30% from the baseline within the first two weeks is considered an acceptable hemodynamic shift and doesn’t require stopping the drug. However, hyperkalemia is a persistent danger. Patients with chronic kidney disease (CKD) or those managed according to the Diabetes Mellitus review standards are at the highest risk. Avoid combining these drugs with potassium-sparing diuretics like spironolactone or potassium supplements unless under strict specialist supervision, as serum potassium levels exceeding 5.5 mEq/L can trigger cardiac arrhythmias.
ACE Inhibitors vs. ARBs: The Key Differences
While both classes target the Renin-Angiotensin-Aldosterone System (RAAS), their mechanisms differ. ACE inhibitors stop the conversion of Angiotensin I to Angiotensin II, but they also prevent the breakdown of bradykinin. This accumulation of bradykinin causes the characteristic dry cough in 5 to 20% of patients and the rare, life-threatening angioedema. Angiotensin II Receptor Blockers (ARBs) provide a direct receptor blockade at the AT1 site and don’t affect bradykinin levels. The 2008 ONTARGET trial demonstrated that while both classes are equally effective for cardiovascular protection, combining them provides no additional benefit and significantly increases the risk of renal dysfunction and hypotension.
Exam Mastery: How to Study ACE Inhibitors for Boards
Mastering the pharmacology of ace inhibitors requires more than memorizing a list of drugs ending in “-pril.” For the 2026 NAPLEX and USMLE Step 1, you’ve got to understand the physiological ripple effects of blocking the Renin-Angiotensin-Aldosterone System (RAAS). Board exams frequently test your ability to predict electrolyte shifts, specifically hyperkalemia, and recognize the classic side effect of a dry, non-productive cough caused by bradykinin accumulation. PharmEDU’s video vignettes simplify these RAAS complexities by visualizing the biochemical pathways. This visual approach makes it easier to recall why these medications are first-line for patients with diabetes and proteinuric kidney disease during high-pressure testing scenarios.
Pharmacology Board Review Strategies
Focus your study time on “Class Effects” first. Most ace inhibitors share a nearly identical side effect profile and therapeutic utility. However, you’ll stand out on shelf exams by knowing the outliers. For instance, Lisinopril and Captopril are the only two members of the class that aren’t prodrugs, meaning they don’t require hepatic activation. This is a common “gotcha” question on clinical exams. Consistent repetition is vital for long-term retention. You can use Pharmacology Flashcards for daily active recall to cement these differences. If you’re preparing for a specific clinical track, the Pharmacology Study Guide for Nursing Students provides targeted insights for your curriculum.
Integrating Clinical Knowledge
Clinical rotations demand practical application of your textbook knowledge. You’ll often need to counsel patients to avoid salt substitutes. Many of these products contain potassium chloride instead of sodium chloride, and combining them with therapy can lead to life-threatening arrhythmias. Pharmacists play a critical role here by screening for drug-drug interactions, particularly with NSAIDs, which can blunt the antihypertensive effect and increase the risk of acute kidney injury. Use this final checklist for your next rotation:
- Confirm pregnancy status, as these drugs are strictly contraindicated due to teratogenicity.
- Monitor for a baseline serum creatinine increase; a rise of up to 30% is often acceptable and expected.
- Screen for a history of angioedema, which precludes the use of this drug class forever.
- Verify that baseline potassium levels are below 5.0 mEq/L before starting therapy.
Success on boards comes from connecting mechanism to manifestation. When you understand the “why” behind the cough or the renal protection, the “what” becomes second nature. Unlock the full PharmEDU library to ace your next exam and gain the confidence you need for clinical practice.
Elevate Your Clinical Competence in Cardiovascular Pharmacology
Mastering the RAAS pathway and these essential antihypertensive mechanisms provides the foundation for managing complex cardiac and renal pathologies. You’ve gained insight into the critical monitoring requirements for 2026 standards, focusing on the early detection of hyperkalemia and the management of bradykinin-related side effects. These high-yield clinical pearls don’t just help you pass exams; they ensure patient safety during real-world interventions. Retention of this information requires a structured approach that fits into a demanding medical schedule.
PharmEdu simplifies this process by offering a comprehensive library of over 100 high-yield pharmacology topics tailored for healthcare students. Our platform integrates interactive flashcards and board-style practice quizzes to reinforce your knowledge through active recall. The mobile-compliant micro-learning modules allow you to turn 10-minute breaks into productive study sessions, ensuring you’re always prepared for the next rotation or board question. It’s time to transform how you approach pharmacological mastery with tools built for your success.
Start your free PharmEDU trial and master ace inhibitors today
We’re excited to support your professional growth as you build the expertise needed to excel in modern medicine.
Frequently Asked Questions about ACE Inhibitors
What is the most common side effect of ACE inhibitors?
A persistent, non-productive dry cough is the most frequent side effect, affecting between 5% and 20% of patients. This occurs because ace inhibitors prevent the breakdown of bradykinin in the lungs, which irritates the respiratory tract. It’s not dose-dependent and typically resolves within 1 to 4 weeks after stopping the medication. Patients who can’t tolerate this often switch to Angiotensin II Receptor Blockers to maintain their treatment goals.
Can ACE inhibitors be used during pregnancy?
No, healthcare providers must avoid prescribing ace inhibitors during pregnancy due to high risks of fetal toxicity and malformations. The FDA classifies these drugs as Category D because they can cause oligohydramnios, skull hypoplasia, and renal failure in the fetus. If a patient becomes pregnant, she should transition to safer alternatives like labetalol or methyldopa immediately. This contraindication is absolute during the second and third trimesters.
How do ACE inhibitors protect the kidneys in diabetic patients?
These medications provide renoprotection by dilating the efferent arteriole, which significantly lowers intraglomerular capillary pressure. By reducing this pressure, they slow the progression of diabetic nephropathy and decrease albuminuria by up to 35% in clinical trials. It’s a standard of care for patients with a urinary albumin-to-creatinine ratio exceeding 30 mg/g. This mechanism helps preserve long-term renal function despite the initial minor rise in serum creatinine.
Why do ACE inhibitors cause a dry cough?
The dry cough results from the accumulation of bradykinin and substance P in the upper airways. Since the angiotensin-converting enzyme normally breaks down these inflammatory mediators, inhibiting it leads to their buildup. This irritation triggers the cough reflex in about 1 in 10 patients. It’s a class effect, so switching to a different medication within the same category won’t solve the problem for the patient if they’re sensitive to it.
What is the difference between an ACE inhibitor and an ARB?
The primary difference lies in their mechanism; ACE inhibitors block the production of Angiotensin II, while ARBs block its binding to the AT1 receptor. Unlike ACE inhibitors, ARBs don’t interfere with bradykinin metabolism, which is why they don’t cause the characteristic dry cough. Studies like the ONTARGET trial show similar cardiovascular outcomes for both classes. Choosing between them often depends on the patient’s specific tolerance for side effects.
What should I monitor when a patient starts an ACE inhibitor?
Clinicians must monitor serum potassium levels, serum creatinine, and blood pressure within 1 to 2 weeks of initiation. A rise in creatinine up to 30% from baseline is often acceptable and reflects the drug’s hemodynamic effect on the kidneys. However, hyperkalemia occurs in approximately 3% of outpatients, requiring dietary changes or dose adjustments. Regular monitoring ensures the patient’s safety while achieving therapeutic goals for hypertension or heart failure.
Are all ACE inhibitors once-daily medications?
Most modern agents like Lisinopril or Ramipril are dosed once daily, but Captopril requires administration 2 to 3 times a day. Captopril has a short half-life of about 2 hours, making it less convenient for long-term adherence compared to newer options. Benazepril and Enalapril typically provide 24-hour coverage with a single dose. Always check the specific pharmacokinetics of the prescribed agent to ensure the patient maintains stable plasma concentrations.
What happens if a patient develops angioedema while on an ACE inhibitor?
You must discontinue the medication immediately and provide emergency medical intervention to maintain the airway. Angioedema occurs in 0.1% to 0.7% of patients and is a life-threatening emergency caused by excessive bradykinin levels. Once a patient experiences this reaction, they should never take any ACE inhibitor again. Medical records must be updated to list the drug class as a major allergy to prevent future accidental exposure.





