Diabetes Mellitus: A Comprehensive Clinical and Pharmacological Review (2026)
What if the key to mastering the complex management of diabetes mellitus isn’t found in memorizing endless drug lists, but in decoding the eight distinct metabolic failures known as the Ominous Octet? Most clinicians and students find it frustrating to distinguish between the nuanced mechanisms of SGLT2 inhibitors and GLP-1 agonists while simultaneously juggling the 2026 diagnostic thresholds for A1C and fasting glucose. It’s easy to feel overwhelmed when a patient’s lab results sit right on the edge of the 6.5% A1C mark or when you’re racing to differentiate DKA from HHS in an emergency setting. You’ve likely felt the pressure of keeping pace with rapidly evolving pharmacological guidelines that change every few years.
This review provides a high-yield framework to help you master these clinical challenges, ensuring you select the right drug class for every patient profile and excel on your pharmacology board exams. We’ll examine the updated 2026 diagnostic criteria, break down the pharmacological pathways of oral hypoglycemics, and provide clear protocols for managing acute hyperglycemic crises. By the end of this guide, you’ll have a structured, evidence-based approach to metabolic care that transforms clinical uncertainty into professional confidence.
Key Takeaways
- Differentiate between autoimmune beta-cell destruction and insulin resistance to refine your clinical diagnostic accuracy and classification skills.
- Apply the updated 2026 standardized diagnostic thresholds for A1C, FPG, and OGTT to ensure precise patient screening and monitoring.
- Master the mechanism-based classification of treatments for diabetes mellitus by mapping pharmacological agents to their primary physiological sites of action.
- Learn to rapidly distinguish between life-threatening acute emergencies like DKA and HHS through high-yield biochemical marker comparisons.
- Enhance patient safety and exam performance by identifying critical drug-drug interactions and essential “Black Box” warnings for common glycemic therapies.
Defining Diabetes Mellitus: Pathophysiology and Classification
Diabetes mellitus isn’t a single disease. It represents a complex group of metabolic disorders where chronic hyperglycemia serves as the defining hallmark. This state of elevated blood glucose results from defects in insulin secretion, insulin action, or both. Understanding the pathophysiology and classification of diabetes mellitus is vital for clinical students because the underlying mechanism dictates the entire therapeutic approach. While we often simplify the condition into two main categories, modern medicine recognizes a much broader spectrum of dysfunction.
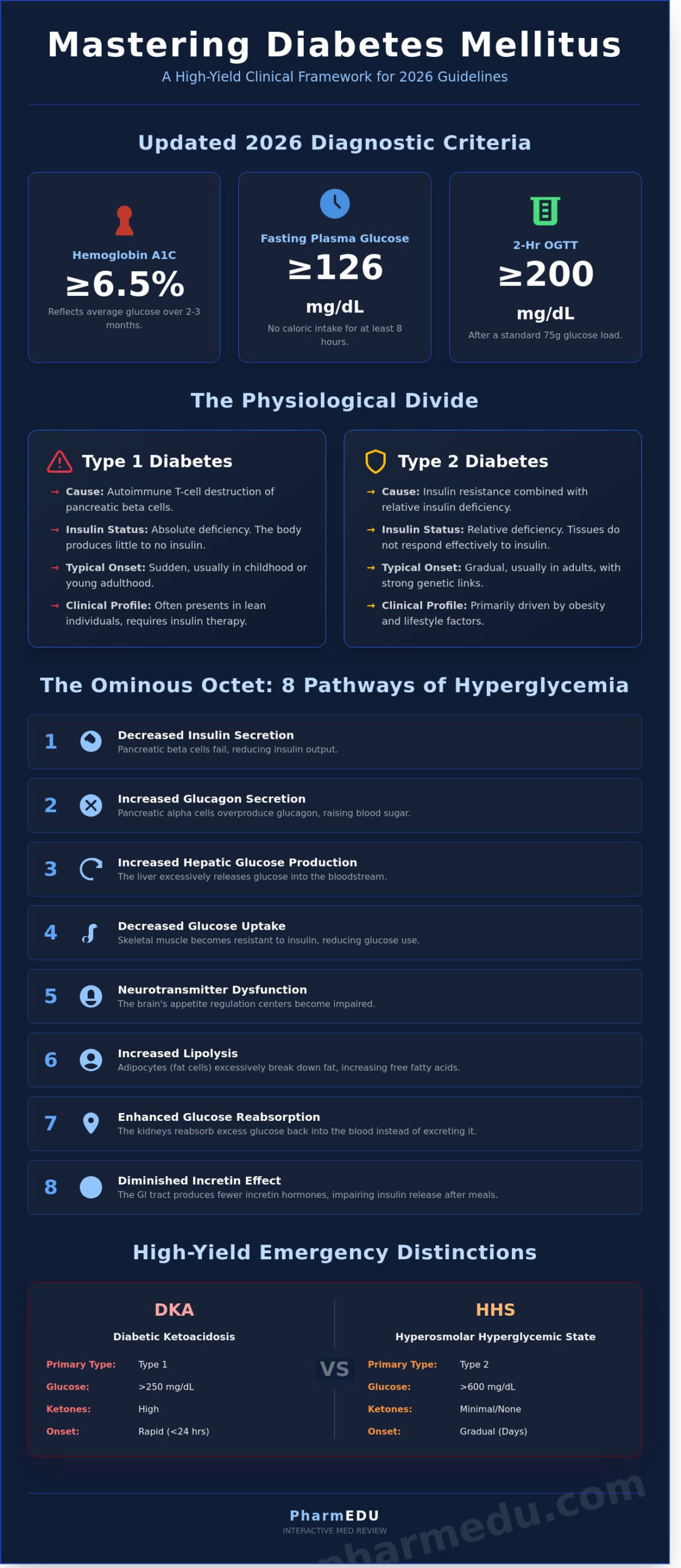
The progression of hyperglycemia involves more than just the pancreas. Ralph DeFronzo identified the “Ominous Octet” in 2009, a framework describing eight distinct physiological pathways that contribute to glucose intolerance. These include:
- Decreased insulin secretion from pancreatic beta cells.
- Increased glucagon secretion from alpha cells.
- Increased hepatic glucose production.
- Decreased glucose uptake in skeletal muscle.
- Neurotransmitter dysfunction in the brain affecting appetite.
- Increased lipolysis in adipocytes.
- Enhanced glucose reabsorption in the kidneys.
- A diminished incretin effect in the gastrointestinal tract.
This multi-organ involvement explains why patients often require combination therapies to achieve glycemic targets. Clinicians are also paying closer attention to Type 3c diabetes, also known as pancreatogenic diabetes. This form arises from exocrine pancreatic diseases like chronic pancreatitis or cystic fibrosis. Studies indicate that up to 9 percent of patients previously labeled as Type 2 actually have Type 3c, which requires specific management of malabsorption alongside glucose control.
Type 1 vs. Type 2: The Physiological Divide
Type 1 diabetes involves an absolute insulin deficiency. It’s typically an autoimmune process where T-cells destroy over 80 percent of the pancreatic beta cells. Genetic markers like HLA-DR3 increase susceptibility, though environmental triggers often precede clinical onset. In contrast, Type 2 diabetes begins with relative insulin deficiency. Here, tissues become resistant to insulin’s signals. While genetics play a stronger role in Type 2 than Type 1, obesity remains the primary driver. Clinical vignettes usually present Type 1 in lean children with sudden onset, while Type 2 appears in older adults with a gradual progression of symptoms.
Secondary and Gestational Classifications
Gestational diabetes mellitus (GDM) occurs in approximately 6 percent of pregnancies in the United States. It’s diagnosed during the second or third trimester and usually resolves after delivery. However, women with GDM face a 50 percent higher risk of developing Type 2 diabetes within 10 years. Secondary diabetes results from external factors. For example, high-dose corticosteroids like prednisone can induce hyperglycemia by increasing hepatic glucose output. Rare forms like Maturity-Onset Diabetes of the Young (MODY) are monogenic, caused by a single gene mutation, and account for less than 2 percent of all cases.
Clinical Presentation and Diagnostic Criteria
The hallmark of a diabetes mellitus diagnosis often begins with the recognition of the classic “3 Ps”: polyuria, polydipsia, and polyphagia. These symptoms result from the osmotic pull of glucose in the renal tubules. When blood glucose levels exceed the renal threshold of approximately 180 mg/dL, the kidneys cannot reabsorb the excess sugar. This leads to glucose excretion in the urine, which pulls significant volumes of water along with it. Patients often report waking up multiple times a night to urinate, followed by an unquenchable thirst and an increase in appetite as the body attempts to compensate for lost calories and fluids.
Early identification hinges on adhering to standardized clinical presentation and diagnostic criteria. According to the 2026 clinical guidelines, a formal diagnosis requires meeting one of the following thresholds, usually confirmed by repeat testing on a separate day:
- Hemoglobin A1C: ≥6.5%
- Fasting Plasma Glucose (FPG): ≥126 mg/dL (7.0 mmol/L) after at least 8 hours of no caloric intake
- Oral Glucose Tolerance Test (OGTT): ≥200 mg/dL (11.1 mmol/L) two hours after a 75g glucose load
Clinicians must prioritize screening for prediabetes, defined by an A1C of 5.7–6.4%, to implement lifestyle interventions that prevent microvascular complications like retinopathy and nephropathy.
The Gold Standard: Understanding A1C
Hemoglobin A1c represents the percentage of hemoglobin that has glucose chemically linked to it. Because red blood cells have a lifespan of roughly 120 days, this test provides a stable, three month average of glycemia. It’s more convenient than fasting tests because it doesn’t require patient preparation. However, certain conditions can skew these results. For instance, sickle cell anemia or recent blood loss can cause falsely low readings due to rapid red cell turnover. Conversely, pregnancy can alter glycation rates, making the A1C less reliable in the second and third trimesters.
Acute Symptoms and Physical Exam Findings
Beyond the 3 Ps, patients often present with unexplained weight loss. This occurs because the body, unable to utilize glucose for energy, begins breaking down fat and muscle tissue. Blurred vision is another common complaint, caused by osmotic changes that swell the lens of the eye. During a physical examination, practitioners should look for Acanthosis Nigricans. This velvety, hyperpigmented skin thickening in the neck or axilla serves as a visible marker of significant insulin resistance. A thorough foot exam is equally vital. Identifying early peripheral neuropathy through monofilament testing can prevent future ulcerations and amputations. Staying current with these exam protocols is easier through accredited professional development modules that focus on evidence based practice.
Screening frequency isn’t universal. While healthy adults should begin screening at age 35 with repeats every 3 years, high risk populations require annual testing. This includes individuals with a BMI over 25 who also possess risk factors such as hypertension, a history of gestational diabetes, or high risk ethnicity. Tailoring the diagnostic approach to the individual’s risk profile ensures that diabetes mellitus is caught in its earliest, most manageable stages.
The Pharmacology of Glycemic Control: Mechanism-Based Treatment
Understanding the pharmacology behind treatment transforms how clinicians approach diabetes mellitus. Modern therapy doesn’t just target blood sugar. It addresses specific physiological sites including the liver, pancreas, gut, kidneys, and skeletal muscle. A deep dive into the pharmacology of glycemic control reveals a clear hierarchy that prioritizes organ protection alongside metabolic stability. Current guidelines have moved beyond simple glucose lowering. They now emphasize cardiorenal protection, especially for patients with established cardiovascular disease or chronic kidney disease.
First-Line Therapy and Biguanides
Metformin remains the gold standard for initial management. It works primarily by activating AMP-activated protein kinase (AMPK). This process decreases hepatic glucose production and enhances insulin sensitivity in muscle tissue. While it’s highly effective, about 25 percent of patients report gastrointestinal side effects like diarrhea or abdominal cramping. Clinicians must also monitor for the rare but serious risk of lactic acidosis in those with reduced renal function. Long-term use is linked to vitamin B12 deficiency in 10 percent of patients, so yearly monitoring is a prudent clinical step.
Incretin Mimetics and SGLT2 Inhibitors
The therapeutic landscape has evolved with the rise of incretin-based therapies and SGLT2 inhibitors. GLP-1 receptor agonists, such as semaglutide, mimic natural hormones to stimulate glucose-dependent insulin secretion and slow gastric emptying. These offer more potent weight loss and cardiovascular benefits than DPP-4 inhibitors, which only prevent the breakdown of existing incretins. The “gliflozin” class, or SGLT2 inhibitors, functions in the proximal tubule of the kidney. By inhibiting glucose reabsorption, these drugs promote the excretion of glucose in the urine. This unique mechanism provides a 35 percent reduction in heart failure hospitalizations and offers significant protection against the progression of diabetic nephropathy.
Insulin Therapy: Kinetics and Delivery
When non-biologic agents can no longer control diabetes mellitus, insulin therapy becomes necessary. Students must distinguish between different kinetic profiles. Rapid-acting insulins like Lispro act within 15 minutes to manage mealtime glucose. Basal insulins like Glargine provide a peakless, 24-hour background level to stabilize fasting numbers. For patients with extreme insulin resistance requiring more than 200 units daily, U-500 concentrated insulin offers a lower-volume delivery option. It’s also vital to account for outside influences like anticholinergic medications. These drugs can significantly delay gastric emptying, which potentially desynchronizes the timing of insulin peaks with glucose absorption from meals.
Managing Acute Complications and Clinical Emergencies
Acute metabolic crises in diabetes mellitus represent life-threatening situations that demand immediate clinical intervention. The two primary emergencies are Diabetic Ketoacidosis (DKA) and Hyperosmolar Hyperglycemic State (HHS). While they share some features, their pathophysiology and biochemical profiles differ significantly, requiring tailored treatment strategies to prevent morbidity.
Clinicians must distinguish these states by evaluating specific biochemical markers:
- pH Levels: DKA presents with metabolic acidosis (pH < 7.30), whereas HHS typically maintains a pH > 7.30.
- Bicarbonate: Levels drop below 18 mEq/L in DKA but remain higher in HHS.
- Ketones: DKA is defined by significant ketonemia and ketonuria; HHS shows minimal or absent ketone production.
Management follows the “SIP” protocol to stabilize the patient systematically. First, Saline (0.9% NaCl) is administered to restore intravascular volume and improve renal perfusion. Second, Insulin is delivered via continuous intravenous infusion (typically 0.1 units/kg/hr) to suppress ketogenesis and lower blood glucose. Third, Potassium monitoring is vital. Because insulin shifts potassium into the intracellular space, clinicians don’t start insulin if serum potassium is below 3.3 mEq/L to avoid cardiac arrhythmias.
Triggers for these emergencies are often predictable. Infection, such as pneumonia or urinary tract infections, accounts for 30% to 50% of cases. Other common causes include medication non-compliance, insulin pump failure, or the onset of new systemic illnesses like myocardial infarction.
DKA: The Acidotic Emergency
DKA occurs primarily in Type 1 patients due to an absolute lack of insulin. This deficiency forces the body to metabolize fat for energy, producing acidic ketone bodies. Patients often exhibit Kussmaul respirations, a deep and labored breathing pattern used to blow off excess CO2. You’ll also notice a distinct “fruity breath” caused by acetone. In pediatric patients, clinicians must be extremely cautious during fluid resuscitation. Rapid shifts in osmolality can lead to cerebral edema, a complication affecting roughly 1% of pediatric DKA cases with high mortality rates.
HHS: The Hyperosmolar Threat
HHS is more common in elderly Type 2 patients and presents with glucose levels often exceeding 600 mg/dL, sometimes reaching 1000 mg/dL. The presence of some residual insulin prevents ketosis but doesn’t stop hyperglycemia, leading to profound osmotic diuresis and dehydration. Patients lose 10% to 15% of their total body weight in fluids. Altered mental status is a hallmark of HHS. While a barbiturate overdose causes central nervous system depression, HHS must remain a primary differential diagnosis for any diabetic patient presenting with lethargy or coma.
Master these emergency protocols and earn your credits through PharmEdu’s accredited clinical training modules.
High-Yield Board Review: Mastering Diabetes for Exams
Success on professional boards requires more than just memorizing drug classes. You must understand how these agents interact within complex clinical scenarios. When managing diabetes mellitus, pay close attention to drug-drug interactions that complicate glycemic control. For example, fluoroquinolones like levofloxacin can cause unpredictable blood glucose swings. Beta-blockers are another high-yield topic because they mask the autonomic symptoms of hypoglycemia, such as tremors and palpitations, though they don’t stop the sweating. Recognizing these nuances is a hallmark of a prepared clinician. Clinicians managing patients with comorbid hyperuricemia should also be aware that certain diuretics used in diabetic patients can precipitate flares requiring specific gout medication management strategies.
Safety remains a top priority for examiners. You must memorize the “Black Box Warnings” for two major classes. Thiazolidinediones (TZDs), including pioglitazone, carry a warning for heart failure because they cause fluid retention. Glucagon-like peptide-1 (GLP-1) receptor agonists are associated with a risk of thyroid C-cell tumors. This makes them contraindicated in patients with a personal or family history of Medullary Thyroid Cancer (MTC). If you’re feeling overwhelmed by these details, the NAPLEX prep course provides a structured framework to help you retain this critical safety data.
To keep insulin types straight, use simple mnemonics. For rapid-acting insulins, remember “LAG” (Lispro, Aspart, Glulisine), which “lag” behind nothing because they’re so fast. For long-acting options, think of “Don’t Go” (Detemir, Glargine, Degludec), signifying they stay in the system for a long duration. Mastering these categories ensures you won’t stumble when a vignette asks for the most appropriate mealtime or basal coverage.
Exam Strategy: Selecting the Best Next Step
Clinical vignettes often ask for the “best next step” in treatment. For a newly diagnosed patient with diabetes mellitus and an A1c under 7.5%, lifestyle modifications and Metformin are usually the correct answer. It’s vital to check renal function first. Metformin is contraindicated if the GFR is below 30 mL/min/1.73m². If the GFR is between 30 and 45 mL/min/1.73m², starting the drug isn’t recommended. For patients with diabetic nephropathy and hypertension, understanding the renoprotective role of ACE inhibitors is essential, as these agents are considered first-line antihypertensive therapy in this population. For acute management, the “Rule of 15” is the standard for hypoglycemia: give 15 grams of rapid-acting carbohydrates and recheck blood glucose in 15 minutes. Repeat until the level is above 70 mg/dL.
Summary of Clinical Pearls
- The Somogyi effect is rebound morning hyperglycemia caused by nighttime hypoglycemia, whereas the Dawn phenomenon is morning hyperglycemia resulting from a natural surge in growth hormone and cortisol.
- Pioglitazone requires 6 to 12 weeks to reach its maximum therapeutic effect because it works through gene transcription via PPAR-gamma activation.
- Sulfonylureas, such as glipizide and glyburide, carry the highest risk of hypoglycemia among oral agents due to their insulin-secretagogue mechanism.
- Always prioritize SGLT2 inhibitors or GLP-1 agonists in patients with established atherosclerotic cardiovascular disease or chronic kidney disease.
Advancing Your Clinical Mastery in Metabolic Care
Effective management of diabetes mellitus in 2026 demands a sophisticated understanding of pathophysiology and the latest pharmacological interventions. Professionals must differentiate between complex clinical presentations and apply mechanism-based treatments to ensure patient safety. Mastering these diagnostic criteria and emergency protocols isn’t just about passing exams; it’s about providing precise care in high-pressure environments. Staying current with these evolving standards requires a structured approach to learning that fits into a demanding medical schedule.
Success in board exams and clinical practice comes from consistent, high-quality preparation. You can Master Pharmacology with PharmEDU Subscriptions to access over 100 high-yield video vignettes specifically designed by healthcare educators. These mobile-compliant micro-learning segments allow you to study efficiently between patient rounds or during a commute. Our platform serves as your digital mentor, bridging the gap between academic theory and practical board exam success. Build the confidence you’ll need to excel in your professional journey and deliver the highest standard of care. Your commitment to continuous growth ensures you’ll stay at the forefront of the medical field.
Frequently Asked Questions
What is the difference between Type 1 and Type 2 diabetes mellitus?
Type 1 diabetes is an autoimmune condition where the body destroys pancreatic beta cells, while Type 2 involves insulin resistance and relative insulin deficiency. Type 1 usually appears in younger patients and accounts for about 5% to 10% of all cases. Type 2 represents 90% to 95% of the diabetes mellitus population. It’s often associated with lifestyle factors like physical inactivity and obesity.
What are the diagnostic criteria for diabetes mellitus in 2026?
The 2026 diagnostic criteria for diabetes mellitus require a fasting plasma glucose of 126 mg/dL or higher or a hemoglobin A1c level of 6.5% or greater. Doctors also use a two hour plasma glucose of 200 mg/dL during an oral glucose tolerance test. These measurements must be confirmed on separate days. If a patient shows classic symptoms of a hyperglycemic crisis, a random glucose of 200 mg/dL is sufficient.
How does Metformin work to lower blood glucose levels?
Metformin lowers blood glucose levels by reducing the amount of sugar the liver produces through the activation of the AMPK pathway. It also increases insulin sensitivity in muscle tissue, improving glucose uptake by approximately 20% to 30%. Because it doesn’t trigger the pancreas to release more insulin, it doesn’t typically cause hypoglycemia. It’s the first line treatment for most patients due to its proven safety profile.
Is Type 2 diabetes reversible through lifestyle changes?
Type 2 diabetes isn’t considered permanently curable, but clinical remission is achievable through significant weight loss and nutritional intervention. Research like the DiRECT trial shows that 46% of participants achieved remission by losing 10 to 15 kilograms. Remission means keeping A1c levels below 6.5% for three months without any medication. It’s a state of metabolic health that requires lifelong management to prevent the return of symptoms.
What happens if diabetes mellitus is left untreated?
Untreated diabetes leads to severe microvascular and macrovascular damage that impacts the heart, kidneys, and nervous system. Roughly 50% of patients with poorly managed glucose develop some form of neuropathy over time. High blood sugar also damages the retina, causing vision loss in 1 out of 3 adults over the age of 40. These complications significantly increase the risk of cardiovascular events like stroke and myocardial infarction.
Can certain medications cause temporary diabetes or hyperglycemia?
Glucocorticoids are the primary medications known to cause temporary hyperglycemia, affecting up to 80% of patients during high dose treatment. Other drugs like thiazide diuretics and certain atypical antipsychotics can also impair insulin sensitivity or secretion. While these effects are often reversible, they can lead to a formal diagnosis if the patient has underlying risk factors. Monitoring is essential for anyone starting these specific pharmaceutical therapies.
What is the primary cause of gestational diabetes during pregnancy?
The primary cause of gestational diabetes is the surge of placental hormones that interfere with the mother’s insulin action. Hormones like human placental lactogen and cortisol increase insulin resistance, peaking between 24 and 28 weeks of pregnancy. Most women can produce enough extra insulin to compensate, but about 6% to 9% cannot. This failure to meet the increased demand results in elevated blood glucose levels for the mother and fetus.
What are the first signs of diabetic ketoacidosis (DKA)?
The first signs of diabetic ketoacidosis include extreme thirst and frequent urination accompanied by blood glucose levels exceeding 250 mg/dL. Patients often experience nausea and abdominal pain within the first 24 hours of the condition’s onset. A fruity breath odor caused by acetone is a specific clinical marker. It’s a medical emergency that requires immediate fluid resuscitation and insulin therapy to prevent life threatening cerebral edema or coma.