
Barbiturate Overdose: Clinical Management and Pharmacology Guide
The clinical assumption that all GABAergic sedatives follow the same safety profile is a dangerous misconception in acute care. Unlike benzodiazepines, which possess a functional ceiling, a barbiturate overdose remains one of the most lethal toxicological challenges because these agents increase the duration of chloride channel opening independently of endogenous neurotransmitters. This pharmacological nuance explains why respiratory failure occurs so rapidly when the GABA-A receptor is over-saturated.
You’ve likely experienced the frustration of trying to memorize the distinct toxicity profiles of short-acting versus long-acting agents during a 12-hour shift or while studying for board exams. It’s easy to feel overwhelmed by the “why” behind specific interventions like urinary alkalization and ion trapping. This guide resolves that confusion. We’ll provide a step-by-step management protocol and the high-yield facts needed for your board certification. You’ll master the precise pathophysiology and the life-saving interventions required to manage these critical patients with confidence and professional precision.
Key Takeaways
- Deepen your understanding of barbiturate pharmacology by mastering the specific mechanism of chloride channel opening and its systemic effects on the CNS.
- Identify the critical clinical markers of toxicity, ranging from respiratory depression to the diagnostic significance of bullous skin lesions in severe cases.
- Master the step-by-step emergency protocols for a barbiturate overdose, focusing on the essential hierarchy of airway management and decontamination strategies.
- Bridge the gap between theory and practice with high-yield comparative tables and insights into cytochrome P450 induction for clinical and exam success.
Understanding Barbiturate Toxicity: Classes, Uses, and Risks
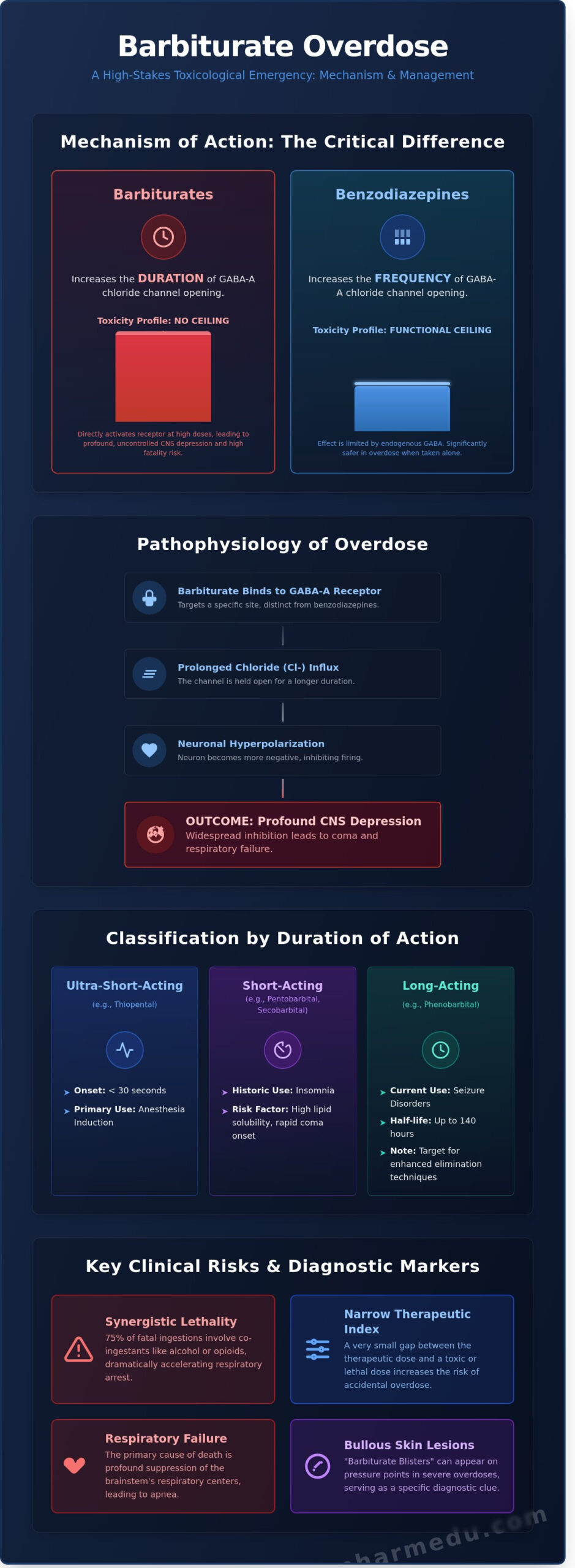
A barbiturate overdose represents a critical medical emergency characterized by profound central nervous system (CNS) depression. These drugs function as positive allosteric modulators of the GABA-A receptor. By binding to specific protein subunits, they increase the duration of chloride channel opening, which leads to neuronal hyperpolarization. Unlike benzodiazepines, which increase the frequency of channel opening, barbiturates can activate the receptor directly at high concentrations. This lack of a pharmacological ceiling creates a narrow therapeutic index, making the risk of fatal respiratory failure significantly higher than with modern sedative alternatives.
Clinicians categorize these agents based on their pharmacokinetic profiles and duration of action. Ultra-short-acting agents like thiopental provide rapid induction for anesthesia, often taking effect within 30 seconds. Short-acting compounds, including pentobarbital and secobarbital, were historically the standard for treating insomnia. Long-acting agents, specifically phenobarbital, remain vital in managing status epilepticus and chronic seizure disorders. While their general use has declined since the 1970s, agents like butalbital are still frequently prescribed in combination products for tension headaches, ensuring these drugs remain a relevant concern in modern toxicology.
The Epidemiology of Barbiturate Misuse
Current trends indicate that while barbiturate prescriptions are less common than in previous decades, the lethality of misuse remains a significant concern for emergency departments. According to data from the 2021 National Survey on Drug Use and Health (NSDUH), millions of adults still misuse prescription sedatives. High-risk populations include patients with chronic seizure disorders and individuals utilizing butalbital combinations for migraines. Statistics show that roughly 75% of fatal sedative-hypnotic ingestions involve co-ingestants. Combining barbiturates with alcohol or opioids creates a synergistic effect that accelerates respiratory arrest, often before medical intervention can begin.
Short-Acting vs. Long-Acting Toxicity
The clinical presentation of a Barbiturate Overdose varies based on the drug’s lipid solubility. High lipid solubility, seen in secobarbital, allows the substance to cross the blood-brain barrier almost immediately, resulting in rapid-onset coma. Conversely, phenobarbital has lower lipid solubility and a slower onset of action. However, its long elimination half-life, which can reach 140 hours in some adults, complicates the recovery process. These long-acting agents are the primary targets for enhanced elimination techniques, such as multidose activated charcoal or urinary alkalinization, because they remain in the systemic circulation for extended periods. Understanding these differences is essential for determining the intensity of supportive care and the necessity of invasive clearance methods.
The Pathophysiology of Overdose: Mechanism of Action
Barbiturates act as potent central nervous system depressants by binding to the GABA-A receptor-chloride channel complex. They target the beta-subunit of the receptor, which is a different binding site than the one used by benzodiazepines. While benzodiazepines increase the frequency of chloride channel opening, barbiturates distinctively increase the duration of each opening event. This prolonged chloride influx results in a more significant hyperpolarization of the postsynaptic neuron, making it less likely to reach the threshold for an action potential. At toxic levels, these drugs don’t just enhance the effects of endogenous GABA; they act as direct agonists of the receptor. This dual action explains why a Barbiturate Toxicity event is often more life-threatening than a benzodiazepine overdose, as the inhibitory effect persists even without GABA present.
GABA-A Receptor Modulation and Chloride Influx
The influx of chloride ions creates a negative membrane potential, which effectively shuts down neuronal communication across large areas of the brain. This widespread inhibition affects the reticular activating system (RAS), the neural network responsible for maintaining wakefulness and consciousness. When the RAS is suppressed, the patient’s level of arousal drops from lethargy to a deep, unresponsive state. GABA-A modulation serves as the primary driver of barbiturate-induced coma.
At high concentrations, the drug’s impact extends beyond GABA receptors. Barbiturates also block excitatory glutamate receptors and inhibit voltage-sensitive sodium channels. These secondary actions contribute to the profound CNS depression observed in a severe barbiturate overdose. The result is a brain that’s pharmacologically “silenced,” leading to the classic presentation of a flat EEG in extreme cases.
The Tolerance Paradox and Respiratory Depression
Patients often develop a rapid tolerance to the sedative and euphoric effects of these drugs, sometimes within 7 to 14 days of continuous use. However, the dose required to suppress the medullary respiratory center remains relatively constant. This “tolerance paradox” means the margin of safety narrows significantly for long-term users, as they require higher doses for the same “high” while the lethal threshold stays the same. Barbiturates blunt the brain’s sensitivity to CO2 levels, leading to hypoventilation and eventual apnea. The loss of the hypercapnic drive is the most common cause of death in these patients.
Beyond the lungs, cardiovascular stability is compromised through several mechanisms:
- Peripheral Vasodilation: Relaxation of vascular smooth muscle leads to significant venous pooling.
- Myocardial Depression: High doses directly reduce the contractility of the heart muscle.
- Hypotension: The combination of vasodilation and reduced cardiac output can cause refractory shock.
In a 2018 clinical review of sedative admissions, cardiovascular complications were present in 22% of severe toxicity cases. Staying updated on these pharmacological nuances is essential for clinical excellence. You can refine your emergency response skills through a professional development course tailored for healthcare providers who manage acute toxicological emergencies.
Clinical Presentation and Diagnostic Evaluation
The clinical hallmark of a barbiturate overdose involves a predictable yet dangerous progression of central nervous system (CNS) depression. Patients typically present with a toxidrome characterized by varying degrees of sedation, respiratory depression, and hypotension. While miosis is often cited in medical literature, pupillary response actually varies; pupils can be reactive, fixed, or even dilated if severe hypoxia has occurred. A unique physical marker to look for is the “barbiturate blister.” These bullous skin lesions occur in roughly 6% of patients with severe toxicity, appearing most often on pressure points or the extremities. Clinicians must recognize that Barbiturate Toxicity Clinical Management requires a high index of suspicion, as physical signs alone can mimic other sedative-hypnotic poisonings.
Identifying the Barbiturate Toxidrome
Symptoms follow a descending path of CNS impairment. Early stages involve ataxia, slurred speech, and nystagmus, which can quickly evolve into flaccid paralysis and deep coma. Monitoring vital signs is critical. Significant barbiturate overdose ingestion often leads to hypothermia and bradycardia due to the suppression of the medullary centers. To help differentiate the cause of CNS depression, clinicians should consider the following:
- Naloxone Challenge: If a patient with respiratory depression doesn’t respond to naloxone, it’s a strong indicator that the cause isn’t opioid-related.
- Reflex Assessment: Deep tendon reflexes are often diminished or absent in severe cases.
- Thermoregulation: Significant hypothermia is more common with barbiturates than with benzodiazepines.
Laboratory Testing and Differential Diagnosis
Standard laboratory workups must include a comprehensive “coma panel” to identify co-ingestants. It’s common for patients to ingest acetaminophen or salicylates alongside barbiturates, which complicates the clinical picture. Standard urine drug screens frequently fail to detect many barbiturates because they’re often calibrated specifically for phenobarbital. Therefore, clinicians shouldn’t rely solely on these screens. Instead, obtain arterial blood gases (ABGs) to assess the depth of respiratory acidosis and metabolic panels to check for organ dysfunction.
Differential diagnosis is essential for safe management. You’ve got to rule out hypoglycemia, acute ischemic stroke, and ethanol poisoning. Serum barbiturate levels provide some guidance, but they don’t always correlate perfectly with the patient’s clinical state. A chronic user might appear relatively functional with a serum level that would be lethal to a non-tolerant individual. Because of this, treatment decisions should focus on the patient’s clinical stability and airway protection rather than just the numerical lab value.
Step-by-Step Clinical Management of Barbiturate Poisoning
The management of a barbiturate overdose begins with the immediate stabilization of vital functions. Airway protection stands as the most critical intervention because respiratory depression is the primary cause of mortality. Clinicians must consider endotracheal intubation if the patient’s Glasgow Coma Scale (GCS) score falls below 8 or if protective airway reflexes are absent. Unlike opioid or benzodiazepine toxicity, no specific pharmacological reversal agent exists for barbiturates. Supportive care remains the cornerstone of treatment. If hypotension persists after a 20 mL/kg bolus of isotonic crystalloids, practitioners should initiate vasopressor support, typically with norepinephrine, to maintain a mean arterial pressure above 65 mmHg.
Immediate Stabilization: Airway and Circulation
Stabilizing the patient requires rapid assessment of breathing and hemodynamic status. You’ll need to monitor oxygen saturation and end-tidal CO2 continuously. While gastric lavage is rarely indicated, administering a single 50g dose of activated charcoal is beneficial if the patient arrives within 60 minutes of ingestion. It’s vital to ensure the airway is protected before administration to prevent aspiration. For long-acting agents like phenobarbital, multi-dose activated charcoal (MDAC) proves effective. This technique interrupts enterohepatic and enteroenteric circulation, effectively “pulling” the drug back into the gut lumen for excretion.
Enhanced Elimination: Urinary Alkalization
Urinary alkalization utilizes the chemical principle of ion trapping to accelerate drug clearance. Since phenobarbital is a weak acid with a pKa of 7.24, increasing the urine pH converts the drug into an ionized form. This ionized state prevents the drug from being reabsorbed in the renal tubules. Clinicians aim for a target urine pH between 7.5 and 8.5. This is achieved by administering an initial bolus of 1 to 2 mEq/kg of sodium bicarbonate, followed by a continuous infusion. You must monitor serum potassium levels closely. Alkalization often induces hypokalemia, which can hinder the effectiveness of the treatment by preventing the kidneys from excreting bicarbonate.
The Role of Hemodialysis
Extracorporeal removal becomes necessary when conservative measures don’t stabilize the patient. Hemodialysis is highly effective for phenobarbital due to its low protein binding (40% to 60%) and small volume of distribution. This procedure can reduce the elimination half-life of phenobarbital from 100 hours to less than 10 hours. Indications for hemodialysis include:
- Serum phenobarbital levels exceeding 100 mg/L.
- Refractory shock or clinical deterioration despite aggressive fluid resuscitation.
- Severe renal or hepatic impairment that prevents natural drug metabolism.
- Persistent metabolic acidosis or electrolyte imbalances.
Short-acting barbiturates don’t respond as well to dialysis. Their high lipid solubility and protein binding mean less of the drug is available in the plasma for removal. In these cases, focus remains on intensive supportive care and preventing secondary complications like pneumonia or pressure sores.
Stay updated on the latest toxicological protocols and earn credits through accredited medical education courses that focus on emergency pharmacology.
High-Yield Board Review: Barbiturates for Students
Mastering the pharmacology of sedative-hypnotics is a prerequisite for success on the NAPLEX and NCLEX exams. While benzodiazepines are more common in modern practice, the unique toxicity profile of barbiturates makes them a favorite for board examiners. You’ve got to distinguish between these classes by focusing on their binding sites and physiological “ceiling effects.”
Essential Mnemonics and Comparison Tables
The most critical distinction lies in the mechanism of action at the GABA-A receptor. Barbiturates increase the duration of chloride channel opening, whereas benzodiazepines increase the frequency. This lack of a biological “ceiling” explains why a barbiturate overdose is significantly more lethal than one involving benzodiazepines alone.
Use the mnemonic B-A-R-B-S to memorize the high-yield side effects frequently appearing in test vignettes:
- Bone loss: Induction of enzymes leads to increased Vitamin D metabolism and subsequent osteomalacia.
- Anemia: Chronic use can cause megaloblastic anemia through interference with folate absorption.
- Rash: Severe cutaneous adverse reactions, specifically Stevens-Johnson Syndrome (SJS), are rare but life-threatening risks.
- Breathing: Profound respiratory depression is the hallmark of toxicity.
- Systemic Induction: They’re among the most potent inducers of the hepatic microsomal enzyme system.
Phenobarbital possesses a pKa of 7.24. This value is close to the physiological pH of 7.4, meaning small shifts in acidity significantly alter the drug’s ionization state. By administering sodium bicarbonate to achieve a urinary pH of 7.5 to 8.0, clinicians trap the ionized drug in the renal tubules to accelerate clearance. Phenobarbital acts as a potent inducer of the CYP450 system, specifically 3A4 and 2C9, which can reduce the serum concentration of co-administered drugs like warfarin or oral contraceptives by 30% to 50% within two weeks of therapy.
How PharmEDU Simplifies Complex Toxicology
Studying for professional licensure requires more than rote memorization. PharmEDU provides high-yield video vignettes that simulate clinical scenarios, helping you recognize the presentation of a barbiturate overdose in a high-pressure testing environment. Our interactive flashcards use evidence-based spaced repetition to help you maintain drug class distinctions long after your initial study session.
The platform functions as a digital mentor, guiding you through the intricate legal and scientific requirements of modern pharmacy practice. You’ll gain access to structured modules that break down complex pharmacokinetic data into actionable clinical knowledge. Master pharmacology with PharmEDU’s comprehensive review to ensure you’re fully prepared for your boards and your professional career.
Mastering Toxicology for Clinical Excellence
Managing a barbiturate overdose requires a precise understanding of GABA-A receptor kinetics and rapid intervention through multi-step clinical protocols. You’ve explored how identifying the specific pharmacological class and implementing urinary alkalinization can reduce complications in critical care settings. These clinical pearls aren’t just vital for patient safety; they’re foundational for your upcoming licensure exams. Navigating the complexities of toxicology becomes much simpler when you have a structured roadmap to follow.
PharmEdu serves as your digital mentor, offering a comprehensive curriculum that covers 100+ distinct therapeutic topics. You’ll find high-yield video vignettes and micro-learning segments designed for busy students who need to maximize their study time without sacrificing depth. It’s the most efficient way to ensure you’re ready for the 250 questions you’ll face on test day. Our platform helps you bridge the gap between academic theory and real-world practice through evidence-based resources.
Ace your boards with PharmEDU’s NAPLEX Prep Course and gain the confidence to excel in your professional journey. You’re well on your way to becoming a trusted healthcare expert.
Frequently Asked Questions
Is there an antidote for barbiturate overdose?
No specific pharmacological antidote exists for this condition. Treatment centers on aggressive supportive care, including mechanical ventilation and fluid resuscitation to maintain hemodynamic stability. Clinical data shows mortality rates for patients requiring ICU admission hover around 2% to 12% depending on the specific agent and co-ingestants. Early intervention remains the most critical factor for a positive patient outcome.
How does phenobarbital differ from other barbiturates in an overdose?
Phenobarbital is a long-acting agent with a half-life of 50 to 120 hours, while short-acting agents like secobarbital have half-lives under 40 hours. This longer duration allows clinicians to use elimination enhancement techniques like urinary alkalization more effectively. Short-acting versions often cause more rapid and severe respiratory failure, making them harder to manage in an emergency setting without immediate mechanical ventilation.
What is the mechanism of urinary alkalization in barbiturate poisoning?
Urinary alkalization works by changing the ionization state of the drug within the renal tubules to prevent reabsorption. By raising the urine pH to a range of 7.5 to 8.5 using sodium bicarbonate, clinicians trap the ionized phenobarbital molecules in the urine. This process increases renal clearance by approximately 5 to 10 fold, which significantly shortens the duration of the coma and respiratory depression.
Can you die from barbiturate withdrawal?
You can definitely die from barbiturate withdrawal if it isn’t managed in a clinical setting. Abrupt cessation after chronic use triggers severe autonomic instability, hyperthermia, and grand mal seizures. Statistics show that roughly 75% of high-dose users experience seizures within 2 to 7 days of their last dose. This mortality risk is significantly higher than that of opioid withdrawal, requiring a slow, medically supervised taper.
How long do barbiturates stay in your system?
Detection times depend on the specific substance’s half-life and the testing method used by the laboratory. Phenobarbital stays in the urine for 14 to 21 days, whereas short-acting barbiturates usually disappear within 2 to 3 days. Blood tests offer a narrower window, typically reflecting use within the last 24 to 48 hours. These windows are extended in patients with renal impairment or those with high adipose tissue.
What is the difference between barbiturate and benzodiazepine overdose?
Barbiturates are significantly more lethal because they don’t require endogenous GABA to open chloride channels. This lack of a ceiling effect means a barbiturate overdose leads to total respiratory arrest and cardiovascular collapse. Benzodiazepines have a much safer profile since they only modulate the frequency of channel opening. This pharmacological distinction explains why barbiturates have been largely replaced by benzodiazepines in modern clinical practice. Understanding these differences is crucial when studying anticholinergic drugs and their mechanism of action, as these agents can present with similar CNS effects but require entirely different management approaches.
What are barbiturate blisters?
Barbiturate blisters are clear, tense skin lesions that form over pressure points or between fingers during a deep coma. They’re seen in about 6% of acute poisoning cases and result from local hypoxia and sweat gland necrosis. These blisters help clinicians differentiate this condition from other types of sedative-hypnotic poisonings during a physical exam, though they aren’t entirely pathognomonic for the drug.
Why is activated charcoal used in barbiturate overdose management?
Multi-dose activated charcoal is used to interrupt the enterohepatic and enteroenteric circulation of the drug. Giving an initial 50g dose followed by 25g every 4 hours can cut the phenobarbital half-life by 50% or more. This technique is a cornerstone of management in a severe barbiturate overdose because it acts as a gut dialyzer. It continuously pulls the drug from the bloodstream back into the intestinal lumen for elimination.





