Cytochrome P450 Explained Simply: A High-Yield Guide for Healthcare Students (2026)
Did you know that a single superfamily of enzymes is responsible for an estimated 80% to 90% of all enzymatic drug metabolism in the human body? If you feel overwhelmed by the alphabet soup of CYP3A4 and 2D6, you aren’t alone. Most healthcare students struggle to keep these pathways straight while preparing for boards or clinical rotations. This article provides cytochrome P450 explained simply, stripping away the academic fluff to give you a clear, high-yield mental model of Phase I metabolism.
We understand that memorizing a random list of inducers and inhibitors feels like an impossible task. We’ll show you how to treat the CYP450 system as a predictable chemical traffic control network instead. You’ll learn to predict drug-drug interactions with confidence and understand exactly how prodrugs fit into the equation. We’ll also cover the latest 2026 updates from the FDA and CPIC, ensuring your knowledge is as current as the newest P450Atlas sequences. By the end of this guide, you’ll be ready to tackle complex pharmacology questions and provide safer patient care.
Key Takeaways
- Understand the “key and lock” binding mechanism and why oxygen and NADPH are essential for fueling metabolic reactions.
- Use intuitive traffic metaphors to distinguish between enzyme inhibitors and inducers without relying on rote memorization.
- Access cytochrome P450 explained simply to navigate the confusing nomenclature of the CYP450 superfamily with ease.
- Learn to safeguard patients by predicting dangerous interactions with narrow therapeutic index drugs like Warfarin and Digoxin.
- Explore how PharmEDU’s interactive flashcards and high-yield video vignettes streamline your preparation for pharmacology board exams.
What is Cytochrome P450? The Body’s Chemical Traffic Control
Think of your liver as a high-security sorting facility. Every drug, toxin, or foreign molecule you ingest eventually arrives here for processing. At the center of this facility is a massive superfamily of enzymes known as Cytochrome P450. To have cytochrome P450 explained simply, you can view these enzymes as the body’s “Garbage Disposal.” Most medications are lipophilic, meaning they dissolve in fats, which makes them difficult for the kidneys to filter. These enzymes chemically modify those substances, making them more water-soluble and preparing them for an easy exit from the body.
The name itself sounds intimidating, but it’s grounded in basic lab science. The “P” stands for pigment, and “450” refers to the 450-nanometer wavelength of light the enzyme absorbs when bound to carbon monoxide. While this is a favorite fact for biochemistry professors, it isn’t essential for your clinical practice. What matters is where they live: primarily in the hepatocytes of the liver, specifically within the smooth endoplasmic reticulum. For a deep dive into the biochemical properties of these heme-thiolate proteins, What is Cytochrome P450? provides a foundational overview. However, for your exams, we’ll focus on how they interact with common medications.
Decoding the Nomenclature: What Does CYP3A4 Actually Mean?
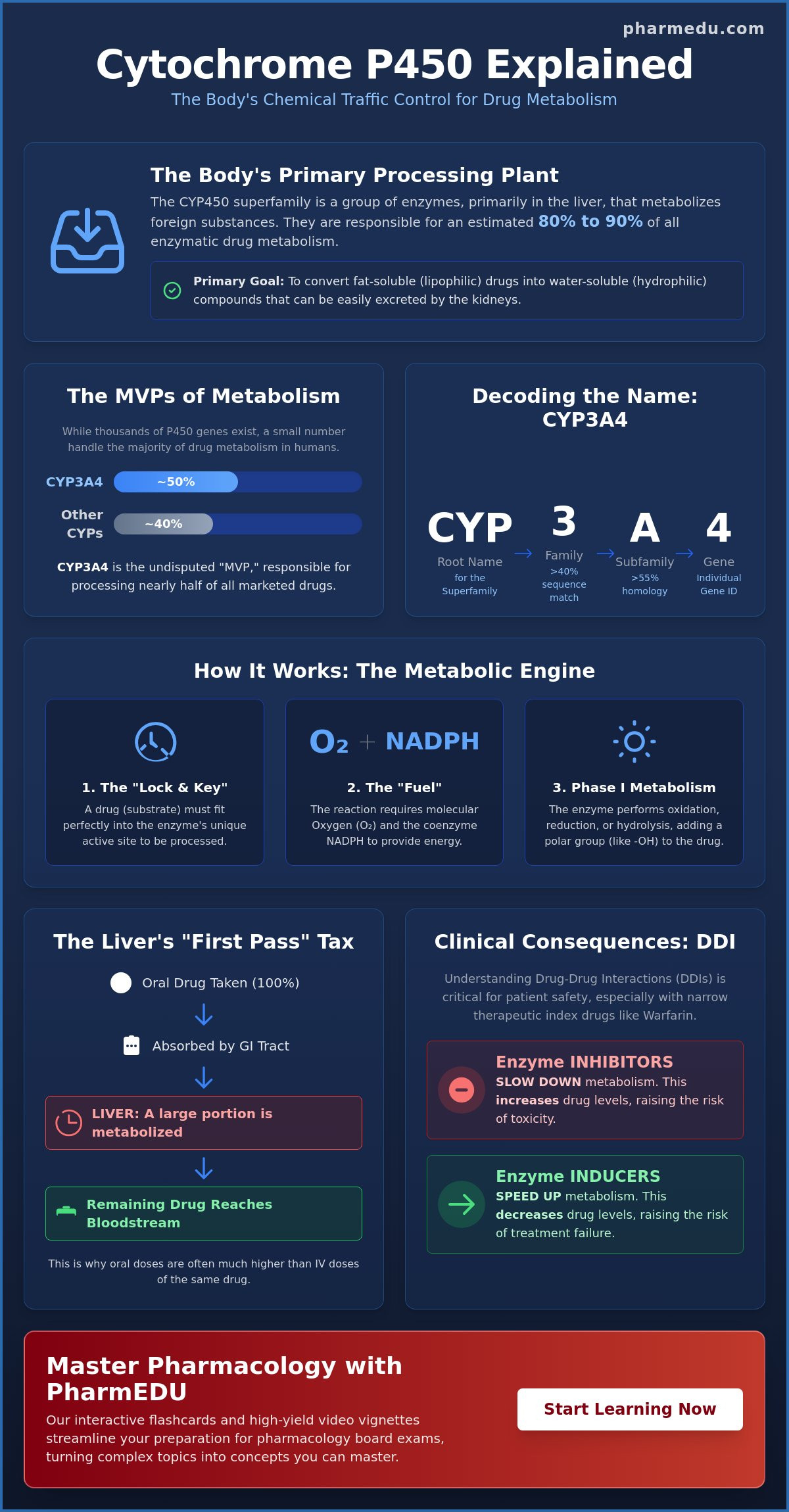
The alphabet soup of enzyme names follows a logical hierarchy. When you see a name like CYP3A4, you’re looking at a biological address. “CYP” is the root name for the superfamily. The first number (3) denotes the family, which includes enzymes that share more than 40% of their sequence. The letter (A) indicates the subfamily, requiring over 55% homology. Finally, the last number (4) identifies the specific gene. While there are over 164,000 known P450 sequences in nature as of 2026, only about a dozen do the heavy lifting in human drug metabolism. Among these, CYP3A4 is the undisputed “MVP,” responsible for processing nearly 50% of all marketed drugs.
The Role of CYP450 in Phase I Metabolism
Metabolism typically happens in two stages. Phase I is the “modification” phase, where CYP450 enzymes perform oxidation, reduction, or hydrolysis. The primary goal is to add or uncover a polar functional group, like a hydroxyl group (-OH). This makes the drug more polar, or water-soluble. While some drugs are fully inactivated here, others are converted into active metabolites. This phase is distinct from Phase II metabolism, which involves conjugation, the process of “sticking” a large, polar molecule like glucuronic acid onto the drug to guarantee it stays water-soluble for kidney excretion. Understanding this distinction is the first step toward predicting how different drugs will behave in your patients.
How the CYP450 System Works: The Mechanism Explained Simply
To have cytochrome P450 explained simply, imagine a highly specific lock and key system. Each enzyme in the superfamily has a unique three dimensional pocket called an active site. When a drug molecule, known as a substrate, enters the body, it must fit perfectly into this pocket to be processed. If the drug’s shape doesn’t match the enzyme’s “lock,” the reaction won’t occur. This specificity is why certain enzymes only handle specific classes of medications, such as statins or beta blockers.
The engine of this system relies on iron, specifically the heme group found at the center of the enzyme. This iron atom acts as a reactive hub that facilitates the transfer of electrons. However, the engine won’t turn over without fuel. The system requires molecular oxygen and a coenzyme called NADPH to provide the necessary energy. Understanding How the CYP450 System Works helps clinicians appreciate why nutritional deficiencies or systemic hypoxia can indirectly impair drug clearance. If you find these biochemical pathways difficult to visualize, our High-Yield Video Vignettes break down these complex interactions into easy to remember animations.
Oral medications face a unique hurdle known as first pass metabolism. After a pill is swallowed and absorbed by the small intestine, it travels through the portal vein directly to the liver. This “first pass” allows CYP450 enzymes to metabolize a significant portion of the drug before it ever reaches the systemic circulation. This is why the oral dose of a drug like propranolol is much higher than the intravenous dose. The liver essentially “taxes” the drug before letting it enter the bloodstream.
The Catalytic Cycle Without the Chemistry Degree
The catalytic cycle is the process of adding oxygen to a drug molecule to change its structure. While textbooks often list seven or more complex electron transfers, you can simplify it into three functional steps. First, the drug binds to the enzyme’s active site. Second, oxygen is activated by the heme iron and NADPH to “attack” the drug molecule. Finally, the newly modified molecule, now called a metabolite, is released. This metabolite is typically more polar and ready for excretion or further processing in Phase II reactions.
Individual Variability: Why We All Metabolize Differently
Not every patient processes drugs at the same speed. This field, known as pharmacogenomics, explains why a standard dose might be toxic for one person but ineffective for another. Genetic polymorphisms can categorize patients into four main groups: poor, intermediate, normal, and ultra-rapid metabolizers. As of April 2026, the Clinical Pharmacogenetics Implementation Consortium (CPIC) has updated guidelines for drugs like ondansetron based on CYP2D6 genotypes. For instance, an ultra-rapid metabolizer might break down codeine into morphine so quickly that they experience respiratory depression, while a poor metabolizer may receive no pain relief at all.
Inducers vs. Inhibitors: Clearing the Confusion
Understanding the interplay between different substances is where pharmacology gets practical. To have cytochrome P450 explained simply, you should view inhibitors and inducers through the lens of traffic management. An inhibitor creates a “Traffic Jam” by blocking the enzyme’s active site, while an inducer builds “Extra Lanes” by increasing the total number of enzymes available. These concepts are the foundation of predicting drug interactions in a clinical setting.
A critical distinction for your exams is the timeline of these effects. Inhibition happens almost immediately because the drug just needs to sit in the enzyme’s pocket to stop it from working. Induction, however, is a slow process. It requires the body to synthesize new proteins, which often takes several days or even weeks to reach a peak effect. For a comprehensive overview of Cytochrome P450 biochemistry, you can see how these molecular changes alter systemic drug clearance over time.
Enzyme Inhibition: The Risk of Toxicity
When an inhibitor enters the system, it competes with other drugs for the same enzyme “lock.” Because the enzyme is busy or blocked, the other drug (the substrate) begins to accumulate in the bloodstream. This leads to levels that can quickly become toxic. A classic clinical example involves grapefruit juice. It contains furanocoumarins that irreversibly inhibit CYP3A4 in the small intestine. If a patient takes a statin with their morning grapefruit juice, the drug’s bioavailability can skyrocket, potentially leading to rhabdomyolysis. You can master these patterns using our Interactive Pharmacology Flashcards, which are designed to make these lists stick.
Enzyme Induction: The Risk of Therapeutic Failure
Inducers work by “revving up” the metabolic engine. By signaling the cell to produce more CYP450 enzymes, these substances cause the body to clear other medications much faster than intended. This creates a risk of therapeutic failure. A famous board exam scenario involves a patient on oral contraceptives who starts taking Rifampin for tuberculosis or St. John’s Wort for depression. The induction of CYP3A4 causes the estrogen to be metabolized so rapidly that it no longer prevents pregnancy.
To keep these straight for your boards, rely on standard mnemonics. For inhibitors, many students use SICKFACES.COM (Sodium valproate, Isoniazid, Cimetidine, Ketoconazole, Fluconazole, Alcohol (acute), Chloramphenicol, Erythromycin, Sulfonamides, Ciprofloxacin, Omeprazole, Metronidazole). For inducers, CRAP GPS (Carbamazepine, Rifampin, Alcohol (chronic), Phenytoin, Griseofulvin, Phenobarbital, St. John’s Wort) is a high-yield tool to ensure you don’t mix up these two opposite forces.
Clinical Consequences: Predicting Drug-Drug Interactions (DDIs)
Predicting interactions requires a systematic approach rather than a collection of disconnected facts. By using the substrate, inhibitor, and inducer framework, you can anticipate how drug levels will shift before the patient even leaves the clinic. To have cytochrome P450 explained simply, you must focus on the “Narrow Therapeutic Index” (NTI) drugs. Medications like Warfarin, Digoxin, and Theophylline leave very little room for error. A minor inhibition of their metabolic pathway can quickly push a patient into the toxic range, while slight induction can render the treatment useless.
Pharmacists serve as the primary gatekeepers of this system, often using sophisticated software to flag these collisions. However, as a clinician, you must understand the logic behind the alert. When a significant interaction is identified, management usually involves one of two paths: adjusting the dose of the substrate or substituting the interacting drug for a “CYP-neutral” alternative. To sharpen your clinical judgment, our Pharmacology Practice Quizzes provide realistic scenarios that mimic the decision-making process found on board exams and in hospital wards.
The Prodrug Trap: When Inhibition Causes Failure
A prodrug is an inactive compound that requires enzymatic conversion to become pharmacologically active. This creates a “paradox” compared to standard drugs. If you inhibit the enzyme responsible for activating a prodrug, the patient experiences therapeutic failure because the active metabolite is never created. The “Codeine Paradox” is a classic example. Codeine requires CYP2D6 to be converted into morphine. If a patient takes a CYP2D6 inhibitor like fluoxetine, the codeine will provide no pain relief. Similarly, the antiplatelet drug clopidogrel requires CYP2C19. Certain proton pump inhibitors (PPIs) can block this pathway, potentially increasing the risk of cardiovascular events in stented patients.
High-Yield Clinical Scenarios for Exams
Exam questions often focus on the direction of change in clinical markers. Consider a patient stable on Warfarin who is prescribed a macrolide antibiotic, a known CYP3A4 inhibitor. Because the metabolism of Warfarin is slowed, the drug accumulates, the INR (International Normalized Ratio) rises, and the patient faces a significant bleeding risk. Conversely, if an epileptic patient on Phenytoin, a potent inducer, starts a new medication, that new drug will likely be cleared faster than expected. Use this 3-step checklist to solve any interaction problem:
- Identify the primary drug: Is it a substrate, a prodrug, or an NTI medication?
- Identify the second drug: Is it a “Traffic Jam” inhibitor or an “Extra Lane” inducer?
- Predict the outcome: Will the active drug level go up (toxicity) or down (failure)?
As of the January 2026 FDA updates, the list of recognized inhibitors and inducers continues to expand. Staying current with these classifications is essential for maintaining patient safety and passing your pharmacology certifications.
Master Pharmacology with PharmEDU’s High-Yield Tools
Mastering the CYP450 system isn’t just about passing a single test. It’s about ensuring patient safety throughout your entire career. We’ve seen how cytochrome P450 explained simply can transform a student’s confidence from confusion to clinical mastery. PharmEDU’s platform is designed to replace traditional, dense textbooks with digital micro-learning strategies that prioritize retention and practical application. Research shows that breaking complex information into smaller, digestible units is the most effective way to retain pharmacological facts under pressure.
Our High-Yield Video Vignettes utilize visual storytelling to make the “key and lock” mechanism unforgettable. We don’t just list facts; we build the mental models you need for clinical rotations. By focusing on high-impact enzymes like CYP3A4 and 2D6, we help you prioritize your limited study time effectively. Our Interactive Pharmacology Flashcards allow you to drill the most common inducers and inhibitors until they become second nature. When you’re ready to test your knowledge, our Pharmacology Practice Quizzes simulate the pressure of board exams, helping you identify and fix weak spots before they matter on a transcript.
Bridge the Gap Between Biochemistry and the Boards
If you need more than just metabolism help, explore our comprehensive pharmacology guide. This resource connects the dots between basic science and clinical practice. For those in specialized tracks, our nursing pharmacology study guide provides targeted insights tailored for the 2026 clinical environment. Universities and teaching hospitals can also secure an Institutional Platform License to provide these high-yield resources to their entire student body, ensuring a standardized level of excellence across the board.
Start Your High-Yield Learning Journey Today
The “explained simply” philosophy is at the core of everything we build. We believe that professional education shouldn’t be a dry, administrative burden. It should be a source of genuine, practical value that supports your professional advancement. Whether you’re a medical student prepping for the USMLE or a pharmacy student facing your final rotations, the right tools make all the difference. Don’t let the complexity of drug metabolism hold you back. Master the material, gain your confidence, and provide the high-quality care your patients deserve. Join PharmEDU and Ace Your Pharmacology Boards today to take the next step in your healthcare career.
Elevate Your Clinical Practice and Ace Your Exams
Mastering drug metabolism is a cornerstone of safe patient care and a vital requirement for your professional credentials. By treating the CYP450 system as a logical network rather than a list to be memorized, you’ve taken the first step toward clinical excellence. You now have cytochrome P450 explained simply, from the mechanics of Phase I oxidation to the complex interplay of prodrug activation and narrow therapeutic index monitoring. These foundational concepts will serve you from your first pharmacology quiz to your final board exams.
Preparation for high-stakes exams like the NAPLEX or NCLEX doesn’t have to be an administrative burden. PharmEDU provides over 100 high-yield video vignettes and mobile-compliant micro-learning segments designed by healthcare educators specifically for your success. Don’t leave your scores to chance. Start Your PharmEDU Subscription and Master Pharmacology Today to turn these complex scientific principles into intuitive clinical skills. You have the potential to excel, and we’re here to provide the structured support you need to reach your goals.
Frequently Asked Questions
Why is CYP3A4 the most important enzyme in the cytochrome P450 system?
CYP3A4 is considered the most significant enzyme because it metabolizes approximately 50% of all commercially available medications. Its high concentration in both the liver and the small intestine makes it the primary gatekeeper for oral drug bioavailability. Because so many different drug classes compete for this specific pathway, it is the most frequent site for clinically significant drug-drug interactions encountered in daily practice.
What is the difference between a substrate, an inducer, and an inhibitor?
A substrate is the specific medication that the enzyme is currently processing or breaking down. An inhibitor acts like a traffic jam, blocking the enzyme’s active site and causing substrate levels to rise to potentially toxic heights. An inducer acts like adding extra lanes to a highway, signaling the body to produce more enzymes so the substrate is cleared much faster than intended. Having cytochrome P450 explained simply through these metaphors helps you predict clinical outcomes.
How does grapefruit juice affect drug metabolism through CYP450?
Grapefruit juice contains natural compounds called furanocoumarins that irreversibly inhibit CYP3A4 enzymes located in the small intestine. This inhibition prevents the “first pass” metabolism of certain drugs, such as specific statins and calcium channel blockers. When this protective metabolic barrier is removed, a much higher concentration of the drug enters the bloodstream, which can lead to severe side effects even at a standard prescribed dose.
Can genetic testing help predict how I will react to certain medications?
Yes, pharmacogenetic testing identifies specific genetic variations that categorize individuals as poor, intermediate, normal, or ultra-rapid metabolizers. For instance, updated April 2026 guidelines from CPIC use CYP2D6 genotyping to personalize the dosing of 5-HT3 receptor antagonists like ondansetron. This data allows clinicians to select the right drug and dose from the start, reducing the risk of therapeutic failure or adverse reactions based on your unique genetic profile.
What happens to a prodrug if the CYP450 enzyme it uses is inhibited?
If the enzyme required to activate a prodrug is inhibited, the patient will experience therapeutic failure because the active metabolite is never created. Unlike standard drugs that become toxic when metabolism is blocked, a prodrug remains in its inactive form. A classic clinical example is codeine. If the CYP2D6 enzyme is inhibited by another medication, the codeine cannot convert into morphine, leaving the patient in pain despite taking the drug.
Is the cytochrome P450 system only found in the liver?
No, while the liver has the highest concentration, these enzymes are also located in the small intestine, lungs, kidneys, and brain. Intestinal enzymes are particularly critical because they begin processing oral medications before they even reach the liver. As of March 2026, researchers have identified over 164,000 P450 sequences across various species, and human research is increasingly focused on how brain-specific CYPs influence local drug responses and neurodegenerative diseases.
How long does it take for an enzyme inducer to start affecting drug levels?
Enzyme induction is a slow process that typically takes several days to two weeks to reach its full effect. This delay occurs because the drug must signal the cell to physically synthesize new enzyme proteins, which takes time. This is a vital distinction from enzyme inhibition, which occurs almost immediately after the drug reaches the enzyme. Clinicians must anticipate this delayed drop in drug concentrations when an inducer is added to a patient’s treatment plan.
Why are narrow therapeutic index drugs so dangerous in the context of CYP450?
Narrow therapeutic index (NTI) drugs, such as warfarin or digoxin, have a very small margin between a dose that heals and a dose that harms. Because these medications are often CYP450 substrates, even a minor change in enzyme activity can lead to a clinical disaster. A small increase in metabolism can make the drug ineffective, while a slight decrease can cause life-threatening toxicity, such as major hemorrhage or cardiac arrhythmias.